ABSTRACT
This study, carried out in a rural community in Ogun state Nigeria, aims to determine the prevalence of soil-transmitted helminths, bacteria causing Chronic Suppurative Otitis Media (CSOM), and their coinfection among school-aged participants. Formol-ether sedimentation technique was used to check for helminth eggs in stool samples. Ear swabs collected were cultured on chocolate, blood and MacConkey agar plates. CD4+T lymphocyte count was derived using a flow cytometre. Study participants were between 5 and 19 years old. Three hundred participants were sampled, 108 (36%) were infected with helminth parasites: Ascaris lumbricoides (28.7%), hookworm (6.7%) and Strongyloides stercoralis (0.7%). The prevalence of helminth infection between the sexes was not statistically significant (χ2 = 0.497; P= 0.390), but statistically significant between the age groups (χ2 = 10.10; P=0.016). Mixed helminthic infections were found in only 3.3% of the study population. Seventeen participants (5.7%) were found to have CSOM. Bacteria isolated in the ear swabs were Pseudomonas aeruginosa, Staphylococcus aureus, Klebiella pneumoniae, Proteus mirabilis and Haemophilus influenzae. Only two percent (2%) of study population were co-infected with helminth and bacteria. Heavy intensity of helminths and heavy growth of bacteria was found in the coinfected when compared with single infected children. This study showed the presence of otitis media in the study area, and that helminthiasis might have an effect on its presentation. Efforts to control CSOM in the study site may need to consider the inclusion of mass deworming.
Key words: Chronic suppurative otitis media (CSOM), helminth, bacteria, coinfection, Ogun State, Nigeria.
Helminth infection is a major cause of disease burden among children in developing countries, especially in sub-Saharan Africa. This burden of helminthic infestations is a direct consequence of acute shortage of health care facilities, lack of access to potable water and sanitation, unhygenic environmental conditions and poverty (Crompton, 2001). Soil-transmitted helminths are parasites causing human infections in tropical and subtropical countries where the eggs or larvae of these parasites thrive in warm and moist soil, and adult worms live in the human gastrointestinal tract for years (Bethony et al., 2006). According to the World Health Organisation (WHO), over a billion people are infected with at least one species (WHO, 2005). Of particular worldwide importance are the roundworms (Ascaris lumbricoides), whipworms (Trichuris trichiura), and hookworms (Necator americanus or Ancylostoma duodenale) (Bethony et al., 2006). They are considered together because children in developing countries can be chronically infected with all three worms thereby causing such children to be malnourished with stunted growth, intellectual retardation and cognitive deï¬cits (WHO, 2005).
Bacteria are causes of infections which range from mild to life threatening. Commensal bacteria in the upper respiratory tract can become virulent and cause serious conditions, such as pneumonia, septicaemia and meningitis. Microbiology cultures of ear discharge in chronic suppurative otitis media (CSOM) often yield multiple organisms which are key etiological agents in the development of CSOM. Common bacteria cultured from the ear discharge includes Pseudomonas aeruginosa, Staphylococcus aureus, Proteus species, Klebsiella pneumonia. Chronic Suppurative Otitis Media (CSOM) is defined as a chronic inflammation of the middle ear and mastoid cavity, which presents with recurrent ear discharges or otorrhoea through a tympanic perforation (WHO, 2004). CSOM remains one of the most common childhood chronic infectious disease worldwide, affecting diverse racial and cultural groups both in developing and industrialized countries, causing considerable morbidity and sometimes leading to extra- and intracranial complications (Trimis et al., 2003).
The infection may occur during the first 6 years of a child’s life reaching a peak around 2 years, and it is commonly found in developing countries in special populations such as children with craniofacial anomalies (Bluestone and Kenna, 1984; Berman, 1995). Infection is also found in certain racial groups (Berman, 1995). The risk of infection with one organism being exacerbated by co-infection with a second species is understudied. An infection may physiologically change the within-host environment in a way that can enhance infection by another bacteria, for example Leishmania spp. creating an ulcerous wound that bacterial opportunists can exploit; and/or infection can cause changes in host immune response for example hookworm-induced suppression of the pro-inflammatory cytokine IFN-g causing increased parasitaemia with Plasmodium parasites (Graham, 2008; Allen and Maizels, 2011). Therefore, a parasitic species encountering an already infected host experiences a different environment than if that host was uninfected. Changes in an infected host’s environment could potentially predispose, or protect, that host from a second infection, and or modulate the intensity of that infection (Celum et al., 2004; Allen and Maizels, 2011).
In a study carried out by Lass et al. (2012), they posited that co-infection is a driver of variation in parasite establishment and growth, ultimately altering the production of parasite transmission stages. In order to test this hypothesis, they divided laboratory mice into three differently infected groups. One group was infected with both self-bioluminescent bacteria (respiratory bacterial pathogen Bordetella bronchiseptica lux+) and intestinal helminth (Heligmosomoides polygyrus) whose egg production was monitored using faecal samples. A second group was infected with H. polygyrus only. They reported a significantly higher bacterial load in the lungs of co-infected animals compared with single infected animals. They also found that five of seven animals in the co-infected groups were super shedders (helminth eggs at a rate 2 s.d.s above single-infected) (Lass et al., 2012). Two or more parasites infecting the same tissue will influence each other directly, or have passive effects or active manipulation of the immune system if colonizing different organs (Cox, 2001). In this study, we aimed to describe the impact of co-infection of helminth parasites and bacteria causing middle ear inflammation. We determined the prevalence of helminth parasites and co-infection with bacteria cultured from middle ear discharge among school aged students.
Study area
This cross-sectional study was conducted in a rural community, Ijoun, in Yewa North Local Government Area of Ogun state located on latitude 7°15/ N and longitude 2°9/ E. The community lacks several basic amenities such as toilet facilities, pipe-borne water, electricity supply, proper waste disposal system and good road network.
Sample size determination
The sample size was determined by the method described by Daniel (1999). Briefly, a prevalence of 16.8% obtained from estimated prevalence of soil transmitted helminths in Ogun State was used (Oluwole et al., 2015). Using a precision of 5% (0.05), a minimum sample size of 215 subjects was computed. Overall, 300 subjects were recruited for the study.
Methodology
Stool samples were analyzed using formol-ether concentration technique (Cheesbrough, 2005), and examined microscopically for helminth eggs or larvae. Sample fluid or pus was collected from the middle ear with a sterile cotton-tipped swab. The swabs collected were immersed in cooked meat media and transported to the laboratory for culture on chocolate, blood and MacConkey agar culture media. Swab samples were inoculated and streaked on the culture media and plates were incubated aerobically at 37°C for 24 h. This was followed by examination of the culture media for any growth which was identified according to standard Microbiology techniques. Venous blood samples (5 mL) were taken from the recruited participants by a medical practitioner. The blood samples were then transferred into an EDTA bottle labelled with the same identification number as the universal bottles used to collect stool samples, and the ones written on the record sheets. The ethylenediaminetetraacetic acid (EDTA) bottles were transported in an EDTA cooling box.
Ethical approval
Ethical approval was obtained from the State Ministry of Health. Written informed consents were obtained from parents of children willing to participate in the study.
Data analysis
The data obtained were summarized using descriptive and inferential statistics with the use of statistical package for social sciences (SPSS), version 20. Prevalence difference across groups was established using chi-square test statistics while intensities and haematological parameters across groups were compared using t-test at α = 0.05.
Prevalence and intensity of helminthiasis
Of the 300 stool specimens examined, 36% showed evidence of helminth infection: A. lumbricoides 28.7%, hookworm 6.7% and S.stercoralis 0.7% (Table 1). A. lumbricoides was the most prevalent helminth infection amongst the infected pupils and was most prevalent among the 5 to 9 years age group (Table 1). The overall mixed infection was 3.3%; a total of 2.7% had dual infection involving Ascaris lumbricoides and hookworm infection, 0.6% had dual infection involving hookworm and S. stercoralis. There was no statistically significant difference between prevalence of helminth infection and the gender of the participants across all age groups but there was a significant difference between the prevalence of helminth infection and the age groups (Tables 2 and 3). The mean number of eggs per gram (epg) of feces for A. lumbricoides and hookworm, in the study population was 7,755±163.67 and 1,142±582, respectively. Analysis of epg of feces by species showed that 15.1 and 10% of the infected participants had heavy intensity of infections for A. lumbricoides and hookworms respectively (Table 4).

Microscopy and culture of ear specimen
Discharge from the middle ear was seen in 29 (9.7%) children (Table 5). A little above half (17(58.6%)) of ear specimens of examined children yielded positive bacteria culture while the remaining 12 (41.4%) showed negative result. Males were more infected than females M:F (1:0.9), the greatest prevalence of infection was observed in the 5 to 9 years age group (75%) (Table 5). Five types of organisms were isolated: Pseudomonas aeruginosa, Staphylococcus aureus, Klebsiella pneumoniae, Proteus mirabilis and Haemophilus influenzae. There was no significant difference between the prevalence of CSOM and gender across the age groups.
Helminth and bacteria coinfection
The overall prevalence of helminth and bacteria (CSOM) co-infection in the study area was 2%. Co-infection of helminth and bacteria was observed only among the 10 to 14 years (2.9%) age group with 3.5% among males, and 0.6% in females (Table 6). Result shows that there was a significant (p < 0.05) difference between the sex of the participant and the prevalence of co- infection in the age group.
Hematological profiles
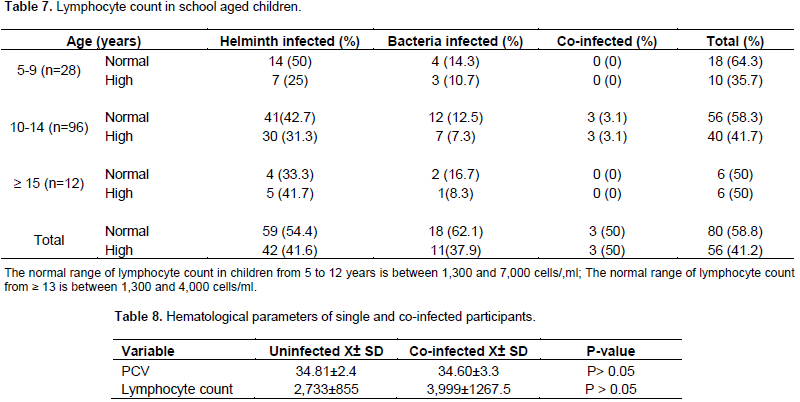
Analysis of haematological profile showed that a total of 41.6, 37.6 and 50% among helminth infected, bacteria infected and co-infected participants respectively were lymphocytotic that is, they had high lymphocyte count (lymphocytes above 7,000/ml for 5 to 12 years and lymphocytes above 4,000 for ≥ 13 years) (Table 7). Analysis of the haematological profile (lymphocyte) among co-infected and uninfected participants showed that there was no significant difference (p >0.05) (Table 8).
The prevalence data observed revealed the prevalence of helminthiasis in the study area as 36%; this is similar to a study carried out in rural areas of southern China where the prevalence of soil transmitted helminths was 36.7% (Shang et al., 2010). Majority of the infections found among the study population were caused by A. lumbricoides and was most prevalent among the 5 to 9 years age group (32.2%), a result similar to the study by Ugbomoiko et al. (2006) in Oba-ile community of Osun state. This could be attributed to indiscriminate defecation and poor hygiene of the children. Hookworm was most prevalent among the ≥ 15 years age group (12.9%). This was close to the observation made by Foghi et al. (2011), in Niger Delta Nigeria who registered that hookworm was more prevalent in the 14 to 16 age group. This could be due to exposure to outdoor activities, poor living conditions and poor hygiene. Intensity data showed that 15.1% of 28.7% of subjects infected with A. lumbricoides had high helminthic load, and 10% of 6.7% infected with hookworm had heavy intensity of infection.
World Health Organisations (WHO) guidelines recommend periodic deworming of children with high intensity infections of 10% and above, regardless of the prevalence rate of helminthic infections. It was observed that 50% of the children who were coinfected had heavy intensity of helminth infection compared with single infected children which was 11.8%. Of the coinfected, 66.7% were found to have heavy growth of the microorganisms causing CSOM when compared with single infection which was 33.3%. Helminth infection causes immunomodulation within the host, there is a skewing of the immune system to Th2 response with widespread anti-inflammatory cytokine network and elevations in interleukin 4 (IL-4), IL-5 and IL-13 (Salgame et al., 2013). This differs from the Th1 mediated inflammatory response (elevated levels of IL-12, IL-23, interferon-γ (IFN-γ) and IL-17) mounted by the immune system in response to bacterial infection
(Gaze et al., 2012).
The contrasting effect on the immune system of both types of infection may reflect in impaired inflammatory response to bacterial infection. In addition, helminths also stimulate very strong regulatory cell populations of both innate and adaptive immune systems. These regulatory cells work through other mechanisms different from Th2 cytokines to down-regulate the Th1 mediated inflammatory responses (Salgame et al., 2013). Though the cytokine profile was not assessed in the study population, it is possible that helminth infection in the participants led to impaired Th1 cytokine inflammatory response with reduced clearance of infecting bacteria from the middle ear and subsequent chronic infection. Evidence of intestinal helminth infection modulating co-infection at a distant site was demonstrated in a study where individuals experimentally infected with hookworm Necator americanus generated strong systemic Th2 response and regulatory T cell response (Gaze et al., 2012).
Efforts to control CSOM in the study site and probably across subSaharan Africa may need to consider the inclusion of mass deworming. Deworming may enhance strong production of IFN-γ following exposure to bacteria antigens (Salgame et al., 2013), and thus help the immune system of the children in controlling bacteria infection in the middle ear In the co-infected group, the presence of high prevalence of participants with multiple species of helminth parasites, heavy growth of bacteria (66.7%) and helminth infection (50%) when compared with the single infected group shows that co-infection can lead to high susceptibility to other infections.
The authors have not declared any conflict of interests.
REFERENCES
|
Allen JE, Maizels RM (2011). Diversity and dialogue in immunity to helminths. Nat. Rev. Immunol. 11:375-388.
Crossref
|
|
|
|
Berman S (1995). Otitis media in children. New England J. Med. 332:1560-1565.
Crossref
|
|
|
|
|
Bethony J, Brooker S, Albonico M, Geiger SM, Loukas A (2006). Soil-transmitted helminth infections: Ascariasis, trichuriasis, and hookworm. Lancet 367:1521-1532.
Crossref
|
|
|
|
|
Bluestone CD, Kenna MA (1984). Chronic suppurative otitits media: antimicrobial therapy or surgery? Pediatr. Ann. 13:417-421.
|
|
|
|
|
Cheesbrough M (2005). District Laboratory Practice in Tropical Countries, Part 1. 2nd edition. Cambridge: Cambridge University Press. P 454.
Crossref
|
|
|
|
|
Cox FEG (2001). Concomitant infections, parasites and immune responses. Parasitology 122:S23-S38.
Crossref
|
|
|
|
|
Crompton DWT (2001). Ascaris and ascariasis. In: Baker JR, Muller R, Rollinson D, eds. Advances in parasitology, 48. San Diego, CA: Academic Press. pp. 285-375.
Crossref
|
|
|
|
|
Daniel WW (1999). Biostatistics: A Foundation for Analysis in the Health Sciences. 7th ed. New York, NY: John Wiley & Sons.
|
|
|
|
|
Foghi BO, Eze NC, Nzeako SO (2011). Helminthiasis in school aged children in a select population in the Niger Delta. Int. J. Trop. Dis. Health 4:793-801.
Crossref
|
|
|
|
|
Gaze S, McSorley HJ, Daveson J, Jones D, Bethony JM, Oliveira LM (2012) . Characterizing the mucosal and systemic immune responses to experimental human hookworm infection. PLoS Pathog. 8:e1002520.
Crossref
|
|
|
|
|
Graham AL (2008). Ecological rules governing helminth-microparasite coinfection. Proc. Natl. Acad. Sci. USA. 105:566-570.
Crossref
|
|
|
|
|
Lass S, Hudson PJ, Thakar J, Saric J, Harvill E, Albert R, Perkins SE (2012). Generating Super-shedders: Co-infection infection increases bacteria load and egg production of a gastrointestinal helminth. J. Royal Soc. Interface 10(80):20120588.
Crossref
|
|
|
|
|
Oluwole AS, Ekpo UF, Karagiannis-Voules DA, Abe EM, Olamiju FO, Isiyaku S (2015). Bayesian geostatistical model-based estimates of soil-transmitted helminth infection in nigeria, including annual deworming requirements. PloS Neglected Trop. Dis. 9(4):e0003740.
Crossref
|
|
|
|
|
Salgame P, Yap GS, Gause WC (2013). Effect of helminth induced immunity on infections with microbial pathogens. Nat. Immunol. 14:1118-1128.
Crossref
|
|
|
|
|
Shang Y, Tang LH, Zhou SS, Chen YD, Yang YC, Lin SX (2010). Stunting and soil transmitted-helminth infections among school-aged pupils in rural areas of southern China. Parasites Vectors 3:97.
Crossref
|
|
|
|
|
Trimis G, Mostrou G, Lourida A, Prodromou F, Syrio-Poulou V, Theodoridou M (2003). Petrositis and cerebellar abscess complicating chronic otitis media. J. Paediatr. Child Health 39:635-636.
Crossref
|
|
|
|
|
Ugbomoiko US, Onajole AT Edungbola LD (2006). Prevalence and intensity of geohelminths infection in Oba-Ile community of Osun State Nigeria. Niger. J. Parasitol. 27:62-27.
|
|
|
|
|
World Health Organisation (WHO) (2004). Chronic Suppurative Otitis Media: Burden of illness and management options; Child and Adolescent Health and Development Prevention of Blindness and Deafness. Geneva: World Health Organization, 2004.
|
|
|
|
|
World Health Organisation (WHO) (2005). Deworming for health and development. Report of the third global meeting of the partners for parasite control. Geneva: World Health Organization, 2005.
|
|