Full Length Research Paper
ABSTRACT
Increased resistance to insecticides and established drugs by malaria vectors necessitate the search for alternative cost-effective malaria control tools in the Ethiopia. Traditional remedies are the most important source of therapeutics of the population and more than 85% of the traditional medical preparations in Ethiopia are of plant origin. As the Ethiopian indigenous medicinal plants' knowledge and diversity is vulnerable to be lost continuous documentation and preservation of traditional knowledge and the plant species is a priority. Thus, we report an ethnobotanical survey of plants traditionally used for malaria prevention and treatment in an indigenous villages of Tepi town south western Ethiopia. To document anti-malarial plant traditional knowledge and determine level of utilization for prevention and treatment of malaria by households, 40 household heads were surveyed by snow ball sampling of which eight household heads addressed by systematic purposive sampling were traditional healers. The data were collected through semi-structured interviews and were analyzed using SPSS version 20. A total of twenty five plant species belonging to twenty two families have been reported. The most cited plant species for malaria prevention by healers were Cyperus species (52.11%), Allium sativum L. (24.15%), Lepidium sativum L. (9.34%) and Echinops kebericho Mesfin. (7.82%). This study has documented more anti-malarial plant species to be used in the indigenous village. The existing medicinal plant species and the indigenous knowledge on traditional medicinal plants in the study area were under serious threat and were at risk of getting lost. Therefore, urgently warrant sustainable conservation and further research is needed.
Key words: Indigenous knowledge, malaria vectors, medicinal plants.
INTRODUCTION
Malaria is a major public health problem in the tropical part of the world, especially in the sub-Saharan Africa. It is estimated that annually there are 300 million cases of malaria worldwide resulting in one million deaths. Ninety percent of these deaths occur in sub-Saharan Africa, and most of the victims are children under 5 years of age and pregnant women (WHO, 2015). Malaria is caused by five species of parasite that affects humans. All the parasites belong to the genus Plasmodium: Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium knowlesi. Of these, P. vivax and P. falciparum are the most important when it comes to the disease propagation of malaria (WHO, 2013).
Malaria is ranked as the leading communicable disease in Ethiopia; it is a leading cause of outpatient visits (17.0%), inpatient admissions (15.0%), and death (29.0%) in most parts of the country (CSA, 2016). It is estimated that more than 85% of the Ethiopian population does not enjoy the services and benefits of modern medicine (Amare, 1976; Dawit, 1986). Moreover, modern drugs are too expensive for the Ethiopian economy particularly the rural mass.
Increased resistance to insecticides by the major malaria vectors (Balkew et al., 2012, Massebo, 2013) and increased spread of drug resistance by malaria parasites (MOH, 2012). Prohibitive costs of the insecticides and drugs necessitate the search for alternative cost-effective methods for malaria control in Ethiopia (Afrane et al., 2008; Deressa et al., 2006).
In malarial infested regions, affordable treatments against malaria are mainly based on the use of traditional herbal remedies. Indeed, indigenous plants play an important role in the management of the disease, and they seem to be the most convenient solution because of their accessibility and diversity in tropical and sub-tropical regions (Karou et al., 2007; Phillipson and Wright, 1991; Ngutaa et al., 2010; Otten et al., 2009; Alemu et al., 2012).
According to several reports, up to 80% of world’s populations still rely on traditional medicine mainly on herbal remedies as primary source of medicinal agents for the treatment of diseases including Malaria (Hostettman and Marston, 2002; Geoffrey and Kirby, 1996). Thus, the development of medicinal plants in primary health care not only will save the foreign exchange but also will aid in conserving our national heritage.
Studies on the anti-malarial plants and their threats in and around Tepi town are limited. Therefore, this study was conducted to document traditional medicinal plant species that are utilized for malaria prevention and treatment and the indigenous knowledge of the people in a native village in south western Ethiopia. Documentation of medicinal plants and the associated indigenous knowledge is very important to conserve the medicinal plant genetic diversity and preserve the knowledge and traditional skills.
MATERIALS AND METHODS
The study area
The study was conducted in an indigenous village of Tepi town Yeki district. The area was purposely selected for this study because it is among the major malaria-prone areas in south west Ethiopia. The villages were selected purposely based on accessibility and knowledge of reported malaria cases. Geographically, the area lies between 7°12’ and 7°43’ W latitude and 35°32’ and 35°75’ E longitude found at 611 km far from Addis Ababa.
The town is bounded by Kefa Zone on east, Mejengir Zone of Gambella region on west, Anderacha district on north, and Sheko district of Bench Maji Zone on south. The altitudinal range of the district falls between 1001 and 2007 m above sea level, and it receives high amount of rainfall, with an average of 1171 to 2200 mm annually. Most households primarily depend on subsistence rain fed agriculture and livestock herding. Malaria control heavily relies on long lasting insecticidal nets (LLINs) and by treatment of diagnosed cases with anti-malarial drugs.
An ethno botanical survey
To document an indigenous anti-malarial plant traditional knowledge and determine level of utilization of traditional medicinal plants for prevention and treatment of malaria by households, 40 household heads were surveyed by snow ball (referral) sampling of which 8 household heads were traditional healers included by purposive sampling. The sample household heads from all-age groups were randomly interviewed from the villages. The ethno-botanical techniques employed to collect data on knowledge and usage of medicinal plants was based on semi-structured interviews and field observation. All plant collections were made by the researchers and field assistant who can speak the local language and also familiar with the traditional healers.
For collection of information on plants used for treating and prevention of malaria by the people living in the study villages, a semi-structured questionnaire was prepared that focus to collect socio-economic status of the participants, local names of the anti-malarial plants, plant parts used, and how such knowledge is preserved and transmitted to next generation. With the help of local informants, the plant species were observed in the field and the plant specimens were taxonomically identified with the help of herbarium materials and experts.
Data analysis
Data collected during the survey was checked by the researcher in the field and after data cleaning, coding and editing; entry and analysis was made using the statistical package for social sciences (SPSS) version 20.0 software. Descriptive statistics mainly frequency and cross tab were employed to analyze the proportion of use-reports of medicinal plant species that were frequently cited by the informants during ethno botanical survey.
Ethical considerations
The objectives of the study were clearly explained and verbal consent was obtained from each study participant. Approval to conduct the study was granted by Mizan Tepi University.
RESULTS AND DISCUSSION
Socio-economic characteristics and knowledge of participants on anti-malarial plants
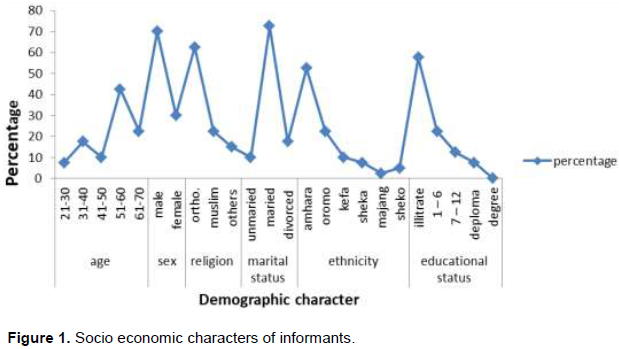
Socio-economic features of respondents are shown in Figure 1. In this ethno-botanical study, majority of the informants who participated in the study were male constitute 70% and female were 30% with an age ranging from 21 up to 70. The majority of the informants were illiterate but many of the respondents had adequate knowledge about traditional anti-malarial medicinal plants that are used for malaria prevention and treatment in their localities.
Traditional usage of anti-malarial plants by households
The present ethno-botanical survey results revealed a total of twenty five plant species used by the local community of Tepi town for prevention of malaria (Appendix 1). As it can be seen the most cited and frequently used plant species and its percentage use for malaria prevention in Tepi town by the villages were: Cyperus species (52.11%), Allium sativum L. (28.15%), Lepidium sativum L. (13.34%) and Echinops kebericho Mesfin (9.82%).
The 25 plant species that were mentioned by the informants as effective against malaria and their uses that were documented during field survey work are provided. The respondents had good knowledge about malaria and could identify it from other fevers on the basis of locally accepted characteristic symptoms that included headache, fever, joint pains, sweating, loss of appetite, thirst, shivering, and bitter taste in the mouth.
Sources of medicinal plants knowledge and preservations
It was found that majority of indigenous knowledge on anti-malarial plants were restricted to elder members with ages ranging from 51 to 60 years and the younger's have limited contribution in this aspect. The majority of the informants responded that the best means of transferring this traditional medicinal knowledge and skill was at the family level. The information has been orally passed down from family members, particularly grandparents and parents. Nonetheless, some traditional healers kept the knowledge with them. The informants' responses indicated that most of the traditional healers were not interested to transfer their knowledge to interested individuals in the community as they may lose their income or recognition in the community.
As a result of accurate knowledge of the plants and their medicinal properties were held by only a few individuals in the community and without exception of indigenous knowledge which was handed down to some elders throughout generation is at risk of getting lost. On the other hand, informants' report showed that the young generation is not eager to acquire the knowledge and skills of the traditional medicinal plants due to the wrong assumption.
Distribution of medicinal plants in the study area
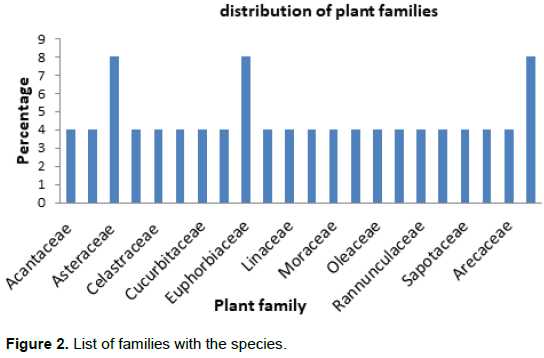
In the study area, a total of 25 plant species distributed into 22 families were identified. These plant species were used for treating malaria ailment. The family Asteraceae, Euphorbiaceae and Brassicaceae accounted for the highest number of medicinal plants composing 2 species (8%) each and the remaining 19 families composing 76%. The species of Asteraceae family used highly for medicinal purpose may be due to their diversified abundance and adaptation to different habitats in which their continuous harvest do not minimize their abundance and most of Asteraceae families are herbs which minimize their destruction for different purposes like trees. The presence of knowledge and practice on medicinal plants by healers shows that the indigenous people of the study area still depend on the traditional medicinal plants (Figure 2).
Habitat variation of medicinal plants
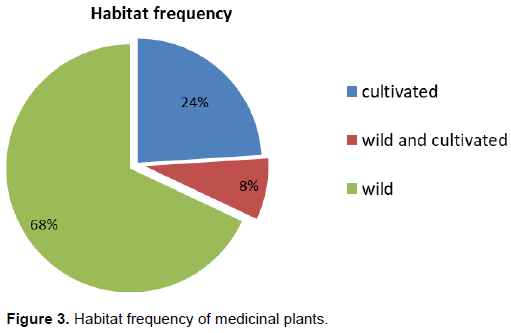
The current finding revealed that most of the medicinal plants obtained from wild 17 (68%) followed by cultivated one 6 (24%). The fact that high number of medicinal plant species was obtained from wilds suggests that the area has good vegetation and wilds are a good option for healers to hide their knowledge from other people which revealed that frequently medicinal plants were collected from the wild in the nearby forest and 68% of the medicinal plants were collected from the natural habitat (Yirga et al., 2011)(Figure 3).
Habitat variation of medicinal plants
The current finding revealed that most of the medicinal plants obtained from wild 17 (68%) followed by cultivated one 6 (24%). The fact that high number of medicinal plant species was obtained from wilds suggests that the area has good vegetation and wilds are a good option for healers to hide their knowledge from other people which revealed that frequently medicinal plants were collected from the wild in the nearby forest and 68% of the medicinal plants were collected from the natural habitat (Yirga et al., 2011)(Figure 3).
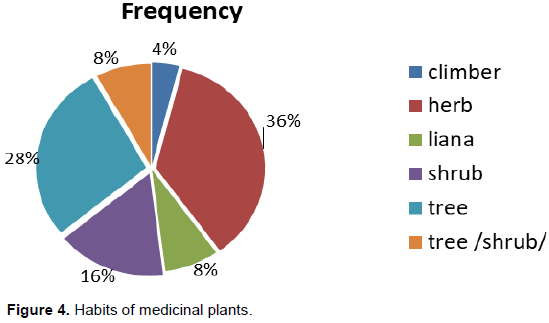
Plant habit
Of the total 25 medicinal plants collected from the study area, 9 (36%) were herb species followed by 7(28%) tree species, 4 (16%) shrubs and 2 (8%) climbers (Figure 4). This shows that most widely used medicinal plants habit in the study area are herbs followed by trees. This may be due to high level of abundance of herb habits in the study area compared to tree and climber species which have less probability of destruction by natural and anthropogenic factors. Relatively high number of herbs and shrubs for medicinal purpose has also been reported previously by Hunde (2004).
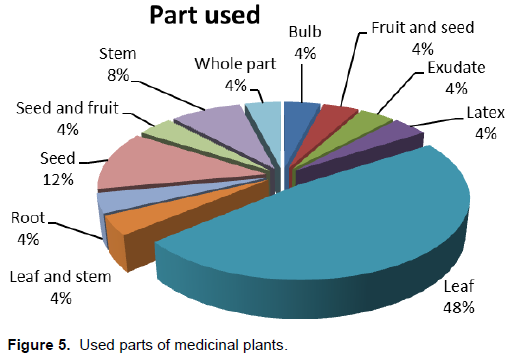
Plant parts used
The most widely used part of plant for the preparation of herbal remedies was leaf 48% followed by seed 12%, stem 8% and the remaining plant parts contribute 4% each (Figure 5).
In the study area, leaf is the most cited plant part in medicine preparation which agreed with reports on medicinal plants by Amenu (2007), whereas, studies in Shirka district (Addis et al., 2001) in northern Ethiopia and in Jabitehnan district western Gojjam (Berhanu, 2002). Since herbal preparation that involves roots, rhizomes, bulbs, barks, stems or whole parts have negative effects on the survival of the mother plants. The fear of destruction of medicinal plants due to the nature of plant parts collected for the purpose of medicine seems to be minimal in the area where this study was conducted. Therefore, the traditional medicine practice has little contribution to destruction of the plant species, because collection of leaves has no greater danger to the existence of an individual plant as compared to the collection of underground parts, stem or whole plant.
Preparation method of medicinal plants
Concerning the preparation of traditional medicine, healers employ various methods of preparation of traditional medicines for malaria treatment. The principal method of traditional medicine preparation reported was squeezing and crushing. This may be due to the possibility of effective extraction of plant ingredients when squeezed or crushed, so that its curative potential would increase.
Preparations may involve using a single plant part or mixtures of different organs of the same plant. In this study, the local people also use some other products as additives in their preparations. For example, water, sugar, salt, milk, and honeys are some of the additives that the local people reported to be used to improve the flavor and reduce adverse effects such as vomiting so that the efficacy of the traditional medicine would be increased. Such additives were also reported by some previous researchers (Abebe, 2001; Giday and Amini, 2003).
Threats to the anti-malarial medicinal plants and indigenous knowledge
In the study area, human and religious factors were found to contribute to the threats that affect medicinal plant species and indigenous knowledge in the study villages. The most serious threat to the existing knowledge and practice on traditional anti-malarial medicinal plants included; agricultural expansion, forest-fire, cultural change, particularly the influence of modernization, accessibility to modern medicine and lack of interests by the younger generations and expansion of protestant religion in which the religious leaders punish healers not to practice were the main problems reported by the informants during the study. Modernization and modification of culture in the area have played a major role in changing the attitude of younger generation to ignore the use of traditional knowledge. Deforestation which is driven by human activities, including agricultural development was reported to be the major threat to the local flora in general and to the anti-malarial medicinal plants in particular.
DISCUSSION
Malaria prevention and treatment
In the study area, traditional medicinal diagnosis is essentially based on systematic interviewing and physical examination if the disease is very serious and the healer thinks that it is the result of evil spirits, magical performances are often carried out to know it clearly. After all, if the healer is unable to ascertain the type of disease, the patient is sometimes referred to the nearby health institution either to bring the result of the diagnosis or to be treated there. The diagnosis of malaria is often simple: intermittent fever and shivering recognized as symptoms of malaria (Dawit Abebe, 1986). The overall conditions of the patient are taken into consideration while measuring out dosages. The major factors that determine whether the treatment is to be given are age, physical fitness, stage of illness, pregnancy and presence or absence of any disease other than the disease to be treated (Dawit Abebe, 1986). For example, drugs that are given through the mouth and the nose are not usually administered to pregnant women unless the patient is in critical situation. Prevention of malaria (as well as other diseases) is commonly practiced by indigenous people using traditional insecticides and insect repellent plants. For example, A. sativum is applied on exposed body parts so as to directly attack mosquitoes and other pathogenic insects.
Smoking and growing medicinal plants near the entrances of the fence is also practiced as insect repellents though detailed information is lacking to how it works. The paired comparison of the five species based on their anti-malarial importance only showed that Cyprus spp. is most preferred followed by A. sativum, L.sativum ranked third for prevention and treatment of malaria.
Conservation of medicinal plants
The direct matrix ranking for randomly selected five medicinal plants used to treat malaria on five uses criteria showed that medicinal plants are widely harvested for different purposes. This is particularly true for E. kebericho Mesfin., Croton macrostachyus Del., Macaranga capensis (Baill) Benth. and Ekebergia capensis Sparm. Thus, indigenous people use those species for charcoal and fire wood. However, Cyprus spp. is extensively used for medicinal purposes by healers only with very little use as fire wood by other people. Generally, the direct matrix ranking shows that those medicinal plants are at conservation risk because of over exploitation and additional uses for different activities.
CONCLUSIONS
The number of medicinal plants reported for the prevention and treatment of malaria is a good indicator of the potential that exists locally so long as scientific procedure is added to the indigenous knowledge. In this connection, it is important to develop the indigenous knowledge by focusing on the most popular plants used against malaria including through extraction and developing phyto medicines. In view of seriousness of malaria in the study area and existence of medicinal plants for the prevention and control of it, research must be enhanced to test activities of those species widely used by the society, namely, A. sativum, C. macrostachyus, L. sativum, Phytolaca dodecandra, Cyprus spp. and E. kebericho Mesfin. Moreover, a further study on the conservation and sustainable use of medicinal plants is recommended.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abebe D (2001). The role of medical plants in health care coverage of Ethiopia, the possible integration. In: conservation and sustainable use of medicinal plants in Ethiopia, proceeding of The National work shop on Bio diversity and sustainable use of medicinal plants in Ethiopia, 28 April. |
|
|
Addis G, Abebe D, Urga K (2001). A survey of traditional medicinal plants in Shirka District, Arsi Zone, Ethiopia, Ethiopian Pharmaceutical Journal 19:30-47. |
|
|
Afrane A, Little J, Lawson W, Githeko K, Yan G (2008). Deforestation and vectorial vapacity of Anopheles gambiae Giles mosquitoes in Malaria transmission, Kenya. Emerging Infectious Diseases 14:1533-38. |
|
|
Alemu A, Muluye D, Mihret M, Adugna M, Gebeyaw M (2012) Ten year trend analysis of Malaria prevalence in Kola Diba, North Gondar, Northwest Ethiopia. Parasites and Vectors 5:173. |
|
|
Amare G (1976). Some common medicinal and poisonous plants used in Ethiopian Folk Medicine (working manual). |
|
|
Amenu E (2007). Use and Management of Medicinal Plants by indigenous People of EjajiArea (ChelyaWereda) West Shewa, Ethiopia: An Ethnobotanical Approach. M.Sc. Thesis. Addis Ababa, Ethiopia. |
|
|
Balkew M, Getachew A, Chibsa S, Olana D, Reithinger R, Brogdon W (2012). Insecticide resistance: a challenge to Malaria vector control in Ethiopia. Malaria Journal 11:13. |
|
|
Berhanu A (2002). Use and conservation of human traditional medicinal plants by indigenous people in JabitehnaWoreda, West Gojjam: with special emphasis to plant species that are used as anti-Malarial treatments, insecticides and insect repellents, (M.Sc thesis, unpublished). |
|
|
Central Statistical Agency (CSA) (2016). The Ethiopian Demographic and Health Survey, Central Statistical Agency, Addis Ababa, Ethiopia. |
|
|
Dawit A (1986). Traditional medicine in Ethiopia: the attempts being made to promote it for effective and better utilization. SINET: Ethiopia. Journal Science 9:61-69. |
|
|
Deressa W, Ali A, Berhane Y (2006). Review of the interplay between population dynamic and Malaria transmission in Ethiopia. Ethiopia Journal Health Development 20:137-144. |
|
|
Geoffrey C, Kirby G (1996). Medicinal plant and the control of protozoa disease with particular reference to Malaria. Transactions of the Royal Society of Tropical Medicine and Hygiene 90:605-609. |
|
|
Giday M, Amini G (2003). An ethno botanical survey on plants of veterinary importance in two weredas of Southern Tigray, Northern Ethiopia. SINET: Ethiopia Journal Science 26(2):123-136. |
|
|
Hostettman K, Marston A (2002). Twenty years of research into medicinal plants: resultsand perspectives. Phytochemistry Reviews 1:275-285. |
|
|
Hunde D (2004). Use and management of Ethno veterinary medicinal plants of indigenous people in Boosat, welenchiti, Ethiopia. Journal. Biological Science 3(2):11-132. |
|
|
Karou D, Nadembega W, Ouattara L, Ilboudo P, Canini A, Nikiéma J, Simpore J, Colizzi V, Traore A (2007). African ethnopharmacology and new drug discovery. Medicinal Plant Science and Biotechnology 1:61-69. |
|
|
Massebo F, Balkew M, Gebre-Michael T, Lindtjorn B (2013). Blood meal origins and insecticide susceptibility of Anopheles arabiensis from Chano in South-West Ethiopia. Parasites and Vectors 6:44. |
|
|
Ministry Health State of Federal Democratic Republic of Ethiopia (MOH) (2012). National Malaria guidelines.3rd edition. Addis Ababa: Commercial Printing enterprise; January, 2012. |
|
|
Ngutaa J, Mbariaa J, Gakuyab D, Gathumbic P, Kiamad S (2010). Anti-Malarial herbal remedies of Msambweni, Kenya. Journal of Ethnopharmacology 128:424-432. |
|
|
Otten M, Aregawi M, Were W, Karema C, Medin A, Bekele W, Jima D, Gausi K, Komatsu R, Korenromp E, Low-Beer D, Grabowsky M (2009). Initial evidence of reduction of Malaria cases and deaths in Rwanda and Ethiopia due to rapid scale-up of Malaria prevention and treatment Malaria Journal 8:14. |
|
|
Phillipson J, Wright C (1991). Can ethno pharmacology contribute to the development of anti-Malarial agents? Journal of Ethnopharmacology 32:155-165. |
|
|
Tamene B (2000). A Floristic Analysis and Ethno botanical Study of the Semi- Wet land of Cheffa Area, South Wello, Ethiopia.M. Sc. Thesis, Addis Ababa University. |
|
|
World Health Organization (WHO) (2015). World Malaria Report, Geneva, Switzerland, 2015. |
|
|
World Health Organization (WHO), (2013). World Malaria Report 2013. |
|
|
Yirga G, Mekonen T, Mezgebe K (2011). Survey of medicinal plants used to treat human ailments in Hawzen district, Northern Ethiopia. International Journal of Biodiversity and Conservation 3(13):709-714. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


