Full Length Research Paper
ABSTRACT
Esophageal cancer is the sixth leading cause of death from malignancies in the world. Given its importance, it is a disease that needs further studies to deepen its understanding and epidemiological behavior. The aim of this work is to evaluate the epidemiological profile of EC in the ABC, Southeast and the national territory of Brazil between 2008 and 2017. This is an ecological study that evaluated the temporal trend of esophageal cancer in the elderly population, between 50 and 79 years of age, between 2008 and 2017 in the ABC region compared to the Southeast region and Brazil as a whole. The number of male hospitalizations has shown an increasing pattern over the years studied in the Southeast and Brazil. The mean number of days of hospitalization tended to decrease for both genders, whereas in the male gender this reduction was expressed in all of the analyzed regions, and in the female gender only in the Southeast and in national scale in Brazil, in a statistically significant way. The average cost of hospitalizations increased in the Southeast and Brazil for males. These findings are important public health markers, which should be considered for the establishment of preventive and health promotion measures for the public network.
Key words: Esophagus, cancer, epidemiology
INTRODUCTION
Esophageal cancer (EC) is the 8th most frequent malignancy in the world. Its worldwide prevalence, in 2012 by the International Agency for Research on Cancer, is estimated at 450 thousand cases; of these, 88% belong to squamous cell carcinoma and about 12% to the type adenocarcinoma (Facina, 2014; Monteiro et al., 2009). It is a neoplasia with a very severe prognosis. This is mainly attributed to the fact that it is usually diagnosed in its later stages: more than 30% of the patients present metastatic dissemination at the time of diagnosis, and virtually no patient is diagnosed with carcinoma in situ. However, it is still one of the less studied types of cancer in the medical literature (Zhang, 2013).
Its dramatic clinical evolution, with a quick local and distance dissemination, and its aggressive treatment both have a great negative impact on the clinical functional status and overall quality of life of the patients affected by the disease (Chang and Church, 2014; Darling, 2013); in addition to high costs per patient for the local health care system (Pinto and Ugá, 2011).
Squamous carcinoma is the most frequent histological type in Brazil and in underdeveloped countries in general. It is more common in men, African descendants and starting after 50 years old. Its classic risk factors are smoking and alcoholism (Henry et al., 2014). Other associations were made with habitual consumption of very hot beverages such as mate, exposure to wood-burning stove smoke, esophageal diseases such as achalasia and Plummer-Vinson syndrome and low socioeconomic conditions (Mota et al., 2013; Gimeno et al., 1995). Some studies highlight the importance of atmospheric and occupational exposure to Aromatic Polycyclic Hydrocarbons (APHs) (Roshandel et al., 2012; Kamangar et al., 2005) produced in the combustion of organic, raw materials of several industries as an important risk factor (Abedi-ardekani et al., 2010; Roth et al., 2009).
Adenocarcinoma is the most common type of EC in developed countries and it is increasing in incidence in the world. It often derives from dysplasia of an intestinal metaplasia called Barret epithelium, in the distal third of the esophagus. It is more common in men, whites and has a higher incidence at more advanced ages: 50 to 70 years of age (Falk, 2009). Its classic risk factors are obesity and gastroesophageal reflux disease (GERD), the main disease responsible for the genesis of Barrett's epithelium, with an increase in its incidence related to the current obesity pandemic and the longer average life expectancy.
Given the importance and epidemiological characteristics of EC described by the international and Brazilian literature, EC needs further studies to deepen its understanding and epidemiological behavior. The metropolitan region named ABC of São Paulo, Brazil, has not yet received its initial description of the epidemiology of the EC. It is a region of great academic interest for this purpose, since it is a well-populated area, a large geographic area, with big heterogeneities in population and geography and having a wide and structured public health network managed by the Unified Health System (SUS) of the municipalities. It also contains a large petrochemical complex located in the municipality of Santo André, with a large population living exposed very close to the burning smoke, generating massive production of PAHs in the inhaled air. The objective of the present study is to evaluate the epidemiological profile of EC in the ABC region between 2008 and 2017 for patients aged 50 to 79 years, comparing this profile with the territories of the Southeast region and national territory of Brazil; besides an analysis of the days of hospitalization and the expenses that this morbidity brings to the municipal SUS of the region.
METHODOLOGY
This ecological study evaluated the temporal trend of esophageal cancer between 2008 and 2017 in the ABC region, composed by seven municipalities, compared to the Southeast region and Brazil. We also evaluated the average costs per individual and total costs in the period, in addition to the average days of hospitalization. These costs comprehended the value for treatment and hospitalization; unfortunately, the database for secondary data does not disclosure the specific treatment type, even so we can have an idea of the cost per individual and its variation by the time.
This study collected data from the Department of Informatics of the Unified Health System (DATASUS). DATASUS is a free access database and represents the main source of health information in the country BRAZIL, 2017.
Esophageal cancer was defined according to the 10th International Classification of Diseases (ICD) as C15.9, which corresponds to malignant esophageal neoplasia. In order to collect data of population, this study used the Brazilian Institute of Geography and Statistics (IBGE), available on the DATASUS website. In the statistical analysis, this study used linear regression models to evaluate the trend of the incidence of this neoplasia, its cost and the days of hospitalization. It was also estimated the trend with the national standard rates for each location and age group, with a confidence level of 95% following the statistical program Data Analysis and Statistical Software for Professionals (Stata) version 11.0®.
RESULTS
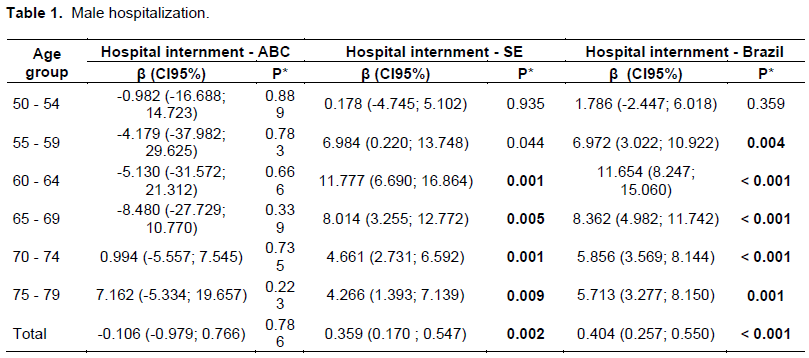
For the male population, there was a statistically significant increase in the gross number of hospitalizations in the Southeast for the age group of 60 to 64 years, 65 to 69 years, 70 to 74 years, 75 to 79 years and for the total hospitalizations in the period, this increase being (95% CI: 1.40, 7.14), and 0.36 (95% CI: 0.75, 95% confidence intervals (CI: 95% CI: 0.17, 0.55). Brazil also observed an increase for this variable in the age groups 55-59 years old of 6.97 (95% CI: 3.02, 10.92), 60-64 years of 11.65 (95% CI: 8.25, 15.06), 65 to 69 years of 8.36 ( (95% CI: 3.57, 8.14), 75 to 79 years of 5.71 (95% CI: 3.28, 8.15), and for the total hospitalizations of 0.40 (95% CI: 0.26, 95% CI: 0.98, 11.74) ; 0.55) (Table 1).
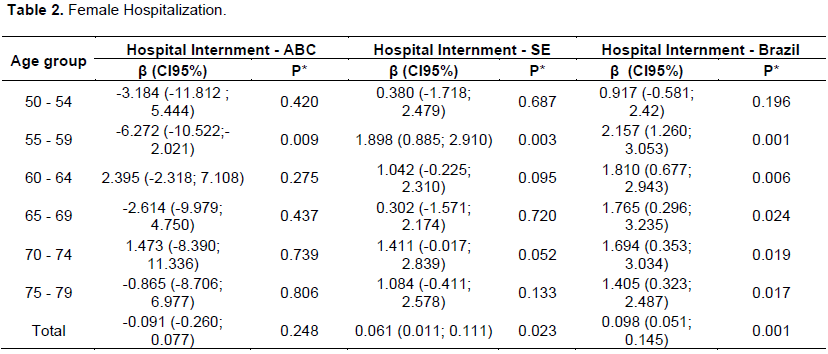
For women, the gross number of hospitalizations increased significantly in the Southeast for the age group 55-59 years old of 1.90 (95% CI: 0.88, 2.91) and for the total number of cases of 0.06 (95% CI: 0.01; 0.11). In Brazil, this significant increase was observed in the age range of 55-59 years in 2.16 (95% CI: 1.26, 3.05), for 60-64 years of 1.81 (95% CI: 0.68, 2.94), 65-69 years of 1.76 (95% CI: 0.35, 3.03), 75 to 79 years of 1.40 (95% CI: 0.32, 2.49) and for the total at 0.10 (95% CI: 0.05; 0.14, 95% CI: 0.29, 3.23) ). For the ABC region, a decreasing trend was observed in the age group 55-59 years old of -6.27 (95% CI: -10.52; -2.02) (Table 2).
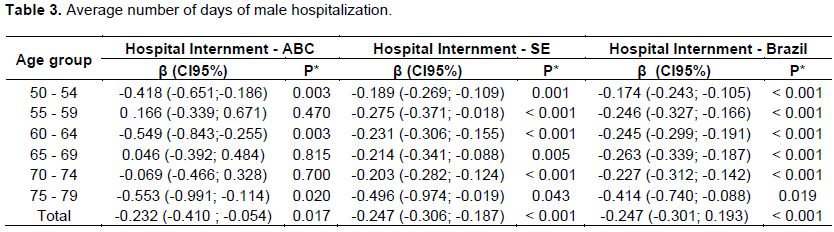
Regarding the average days of hospitalization for each male patient, we observed that, in general, there was a decreasing trend for the three regions. For the ABC region, this decrease was significant for the age group of 50-54 years old of -0.42 (95% CI: -0.65; -0.18, p = 0.003), for 60-64 years of -0.54 (95% CI: -0.84; (95% CI: -0.99, p = 0.003), and for the total cases of -0.23 (95% CI: -0.41; -0.05, p = 0.017). Both Brazil and the Southeast had a decreasing and significant trend for all age groups, and for all ages, this decrease was -0.25 (95% CI: -0.31, -0.19, p <0.001) for the Southeast and -0.24 (95% CI: -0.30; 0.19, p <0.001) for Brazil (Table 3). For women, this variable did not change statistically and significantly in the ABC region, while for the Southeast all age groups, except for 65 to 69 years, decreased, with the total number of cases declining by -0.33 (95% CI, : -0.45; -0.21, p <0.001). For Brazil, all age groups decreased, with the total number of cases declining by -0.32 (95%CI: -0.41; -0.23, p <0.001) (Table 4).

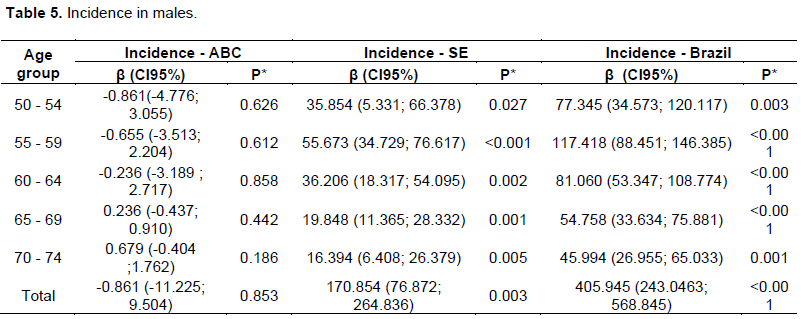
The incidence of esophageal cancer presented an increasing and significant trend for all age groups in the Southeast, with the total number of cases in this region increasing by 170.85 (95% CI: 76.87, 264.84, p = 0.003).
In Brazil, a similar fact was observed, with the exception of the 50 to 54 year age group, in which growth was not significant; the total number of cases in Brazil increased by 405.94 (95% CI: 243.05, 568.84, p <0.001) . However, the ABC region did not change significantly in incidence (Table 5). In females, the incidence of this neoplasia also showed a growing tendency for the Southeast, in the age groups of 55 to 59 years, 60 to 64 years, 70 to 74 years and for the total of cases: there was an increase of 37.62 (95% CI: 9.12, 66.12, p = 0.016). For Brazil, an increase in all age groups was observed, except for men, for the age group 50-54 years, the increase for the total number of cases was 114.76 (95% CI: 59.97, 169.54, p = 0.001) (Table 6).

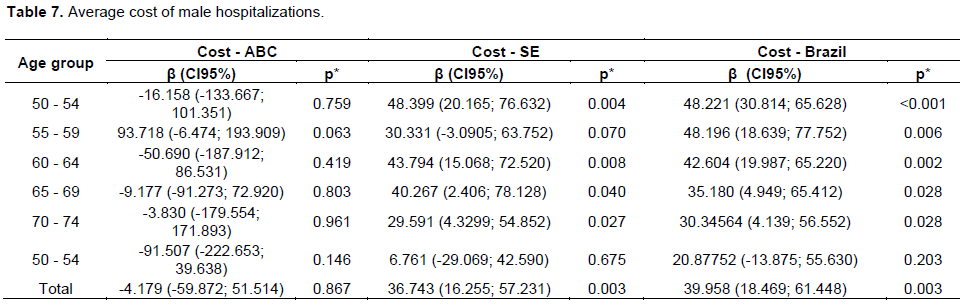
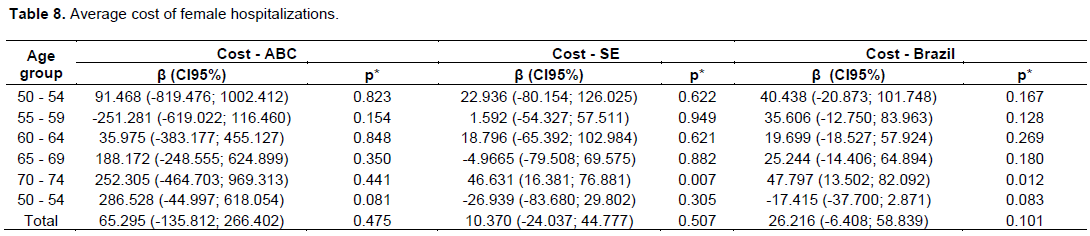
The average cost of admissions for men did not change significantly in the ABC region. For the Southeast this variable had an increasing tendency for the age groups of 50 to 54 years, 60 to 64 years, 65 to 69 years, 70 to 74 years and for the total of all the cases, an increase of 36.74 (95% CI: 16.25, 57.23, p = 0.003). For Brazil, only the age group of 75 to 79 years did not increase its average cost; the total of all age groups in Brazil increased by 39.96 (95% CI: 18.47, 61.45, p = 0.003) (Table 7). In the case of women, a similar fact was observed, with no significant changes in cost in ABC; while in the Southeast there was an increase for the age groups of 55-59 years, 60-64 years, 70-74 years and for the totality of cases, the latter was 37.62 (95% CI: 9.12, 66.12, p = 0.016). In Brazil, there was also an increase, with the exception of the age group from 50 to 54 years; for the total number of cases, this increase was of the order of 114.76 (95% CI: 59.97, 169.54, p = 0.001) (Table 8).
DISCUSSION
When analyzing the epidemiological profile of EC in the region of ABC, Southeastern Brazil, and Brazil, between 2008 and 2017, for patients aged 50 to 79 years, we observed that:
(i) The number of male hospitalizations has shown an increasing pattern over the years studied in the Southeast and Brazil;
(ii) The mean number of days of hospitalization tended to decrease for both genders, whereas in the male gender this reduction was expressed in all the analyzed regions and in the female only in the Southeast and Brazil in a statistically significant way;
(iii) The average cost of hospitalizations increased in the Southeast and Brazil for males.
Cancer is one of the leading causes of death in the world. The number of cancer cases and deaths is expected to grow rapidly as populations grow, age, and adopt lifestyle behaviors that increase cancer risk (Torre et al., 2016). Thus, while Brazil undergoes an epidemiological transition, we observe that infectious-parasitic diseases have their place occupied by chronic diseases, such as cancer. The incidence of esophageal adenocarcinoma
has increased greatly in the last 40 years. Many studies have suggested that the concomitant epidemic of obesity may explain at least part of this increase. The risk of adenocarcinoma may be higher in men because of gender differences in tobacco use or types of obesity, since the prevalence of abdominal obesity is higher among men as well as smoking. It is likely that the etiology of the difference in the sexes is multifactorial, with a differential distribution of some risk factors that lead to the increase of this neoplasia in the male gender (Rubenstein and Shaheen, 2005).
The treatment of esophageal cancer depends on the characteristics of the patient and the tumor, mainly its staging; early tumors may be suitable for endoscopic removal, while more advanced cancers locally are treated with chemotherapy, radiation therapy, surgical resection, or combinations of those (Smyth et al., 2007). There are no current articles that tell us about the average number of days a patient is hospitalized for such morbidity. In this study, we observed a tendency to reduce the number of days of hospitalization. The data that is expressed in all regions analyzed in males may be related to the extension of the country's Unified Health System.
These reductions in days of hospitalization can be explained by some interesting facts that occurred broadly in the recent years. The advanced nutrition therapy, with new features such as body composition analysis and laboratorial and function tests, was proved benefic for almost all patients in the pre-operative and post- operative status and reduced the complications after surgery, which means fewer days of hospitalization (Kondrup et al., 2003; Rotovnik-Kozjek and Milosevic, 2008; Van Bokhorst-de van der Schueren et al., 2012). In addition, the better understanding of the disease course and its poor outcome by the medical team and patients provided a greater adherence to palliative treatment, which reduced the hospitalization days due to advanced home care planning (Reymond et al., 2018).
The increase in the average cost of hospitalizations in the Southeast and Brazil for males can be explained by different ways. The Southeast is the strongest financial region in Brazil, which has the best heath access with modern public hospitals, funded by this region. These reflect in expensive costs with new treatments. The increase in Brazil, as a whole, on the other hand, confirms the better economic status of the National Health System, which consolidated the treatment and finance in poorly regions (Aith et al., 2014). On the other hand, the ABC region decreased its cots by improving the referencing system, in which the patient received his diagnoses in the ABC region, but the treatment is delegate for other more structured regions, such as São Paulo capital (Ugá et al., 2003).
CONCLUSION
In this study, the average number of days of hospitalization tended to decrease significantly for both sexes, and in males. This reduction was expressed in all the analyzed regions, and in females only in the Southeast and Brazil. The average cost of hospitalizations increased in the Southeast and Brazil for males. These facts are important public health markers that should be considered for the establishment of preventive and health care promotion measures for the local public health network.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Abedi-Ardekani B, Kamangar F, Hewitt SM, Hainaut P, Sotouddeh M, Dawsey SM (2010). Polycyclic aromatic hydrocarbon exposure in oesophageal tissue and risk of oesophageal squamous cell carcinoma in north-eastern Iran. Gut 59(9):1178-1183. |
|
|
Aith F, Bujdoso Y, do Nascimento PR, Dallari SG (2014). The principles of universality and comprehensiveness of SUS from the perspective of the rare disease policy and technological incorporation. Revista de Direito Sanitário 15(1):10-39. |
|
|
Chang D, Church J (2014). Evaluating the health-related quality of life of esophageal cancer patients. Practical Radiation Oncology 4(3):181-186. |
|
|
Darling GE (2013). Quality of life in patients with esophageal cancer. Thoracic Surgery Clinics 23(4):569-575. |
|
|
Facina T (2014). Estimate 2014 - incidence of cancer in Brazil. Revista Brasileira de Cancerologia 60(1):63-64. |
|
|
Falk GW (2009). Risk factors for esophageal cancer development. Surgical Oncology Clinics 18(3):469-485. |
|
|
Gimeno SGA, Souza JMP, Mirra AP, Correa P, Haenszel W (1995). Risk factors for cancer of the esophagus: A case control study in a metropolitan area of South-Eastern Brazil. Revista de Saude Publica 29(3):159-165. |
|
|
Henry MACA, Lerco MM, Ribeiro PW, Rodrigues MAM (2014). Epidemiological features of esophageal cancer. Squamous cell carcinoma versus adenocarcinoma. Acta Cirurgica Brasileira 29(6):389-393. |
|
|
Kamangar F, Strickland PT, Pourshams A, Malekzadeh R, Boffetta P, Dawsey SM (2005). High exposure to polycyclic aromatic hydrocarbons may contribute to high risk of esophageal cancer in northeastern Iran. Anticancer Research 25(1):425-428. |
|
|
Kondrup J, Allison SP, Ellia M, Vellas B, Plauth M (2003). ESPEN Guidelines for Nutritional Screening. Clinical Nutricional 22(1):415-421. |
|
|
Monteiro NML, Araújo DF, Bassetti-Soares E, Vieira JPF, Santos MRM, Júnior PPL, Delgado TSJ (2009). Esophageal cancer: Profile of clinical manifestations, histology, location and metastatic behavior in patients undergoing cancer treatment at a referral center in Minas Gerais. Revista Brasileira de Cancerologia 55(1):27-32. |
|
|
Mota OM, Curado MP, Oliveira JC, Cardoso DMM (2013). Risk factors for esophageal cancer in a low-incidence area of Brazil. Sao Paulo Medical Journal 131(1):27-34. |
|
|
Pinto M, Ugá MAD (2011). Cost of treating patients with smoking history in a specialized cancer hospital. Revista de Saude Publica 45(3):575-582. |
|
|
Reymond L, Parker G, Gilles L, Cooper K (2018). Home-based palliative care. Australian Journal of General Practice 47(11):747-752. |
|
|
Roshandel G, Semnani S, Malekzadeh R, Dawsey SM (2012). Polycyclic Aromatic Hydrocarbons and Esophageal Squamous Cell Carcinoma-A Review. Archives of Iranian Medicine 15(11):713. |
|
|
Roth MJ, Wei WQ, Baer J, Wang CQ, Stemberg LR, Warner AC, Johnson LL, Cherry J (2009). Aryl hydrocarbon receptor expression is associated with a family history of upper gastrointestinal tract cancer in a high-risk population exposed to aromatic hydrocarbons. Cancer Epidemiology and Prevention Biomarkers 18(9):2391-2396. |
|
|
Rotovnik-Kozjek N, Milosevic M (2008). Priporocila za prehransko obravnavo bolnikov v bolnisnicah in domovih za starejse obcane. Ljubljana. Ministrstvo za zdravje. |
|
|
Rubenstein JH, Shaheen NJ (2005). Epidemiology, diagnosis, and management of esophageal adenocarcinoma. Gastroenterology 149(2):302-317. |
|
|
Smyth EC, Lagergren J, Filzgerald RC, Lordick F, Shah MA, Lagergren P, Cunningham D (2007). Oesophageal cancer. Nature Reviews Disease Primers 3(1):1-27. |
|
|
Ugá MA, Piola SF, Porto SM, Vianna SM (2003). Decentralization and allocation of resources within the scope of the Unified Health System (SUS). Ciência and Saúde Coletiva 8(1):417-437. |
|
|
Torre LA, Siegel RL, Ward EM, Jemal A (2016). Global cancer incidence and mortality rates and trends - An update. Cancer Epidemiology and Prevention Biomarkers 25(1):16-27. |
|
|
Van Bokhorst-de van der Schueren M, Soeters PB, Reijven PLM, Allison SP, Kondrup J (2012). Diagnosis of malnutrition - Screening and assessment. Basics in Clinical Nutrition (2004):11-18. |
|
|
Zhang Y (2013). Epidemiology of esophagealcancer. World Journal of Gastroenterology 19(34):5598. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


