ABSTRACT
The main cause of diabetes mellitus type 2 (DM2) is disturbed carbohydrate metabolism indicated by hyperglycemia. Insulin secretion is disturbed by inflammatory process in the body due to imbalanced diet, hormonal disturbance and genetics. The serum sialic acid has been investigated as a parameter to evaluate intensity of DM2. 200 individuals of both genders were included and were divided into four groups (50 each) which include; Group 1, the control; Group 2, diabetics without complications; Group 3, diabetics with renal complications and Group 4, diabetics with renal complication and retinopathy. All the blood components were estimated by using enzymatic kits. Body mass index (BMI) was also estimated. It was observed that serum sialic acid (mg%) showed significantly higher (P< 0.01) values in diabetics than control and all other risk factors. All other parameters revealed significantly higher differences than control group with diabetic complications. The present findings indicated that elevated serum sialic acid levels predict renal function disturbance. The serum sialic acid may be taken as a strong predictor of renal dysfunction in diabetes.
Key words: Sialic acid, triglycerides, cholesterol, nephropathy, retinopathy, body mass index (BMI).
Diabetes mellitus type 2 (DM 2) is diagnosed by hyperglycemia and is a result of disturbed carbohydrate metabolism due to abnormal insulin secretion and is also associated with several micro vascular complications. DM is controlled by the hormone insulin from beta cells of Langerhans which secrete insulin according to metabolic needs but deviation from normal insulin secretion due to any reason results in raised serum glucose level and leakage in urine when serum glucose exceeds 180 mg% (Guyton and Hall, 2016). During the last few decades, DM2 has become very common in human beings around the world due to dietary errors or physiological deviations. Only in USA more than 16 million Americans have DM type 2 (Mehta et al., 2009). In India, diabetics were 40.6 million in 2006 which is expected to go up to 79.4 million by the year 2030 (Pradhan et al., 2001; Ghosh et al., 2016). In addition to this, a great percentage is not aware if they are diabetic. It is proposed that urine and blood sugar should be tested at least once in 6 months so that the disease may be handled in its primary stages (Ghosh et al., 2016).
The diabetic complications may result as cardiovascular diseases, kidney nephropathy, retinopathy or other debilitating diseases (Pickup et al., 1997). There are several metabolites in the body including elevated serum sialic acid which may indicate the presence of DM 2 including raised lipid profile, uric acid or delayed wound healing and are also related with cardiovascular diseases. In this study we have focused serum sialic acid (SA) comparison with other diabetic indicators because sialic acid has been reported as a risk factor depicting acute inflammatory changes in the cell membrane and its damage leading to ischemia in blood vessels, kidney, eyes and brain (Yarema, 2006). It is formed by glucosamine in association with acetyl-L-carnitine (acetyl CA). SA is represented with the formula C11H19NO9. It is also known as N-acetyl neuraminic acid, the predominant sialic acid found in mammalian cells with a molecular weight of 309.2699 gM-1 (1 mM = 2.709 mg%) (Chen et al., 1996).
The kidney nephropathy with raised Hemoglobin A1c (HbA1c) and other complications such as retinopathy are also common complications of DM 2. Obesity is also a complication of diabetes or vice versa. Among all parameters which indicate status of DM 2, the raised serum sialic acid is an acute reactant of inflammation resulting from elevated blood sugar levels (Ghosh et al., 2016; Cohen et al., 1981). The increased insulin resistance and lower serum sialic acid contents indicate their association with neuramidase biosynthetic enzyme in DM 2 which is indicative of reduced responsiveness to insulin (Salhanick and Amatruda, 1988). The study was undertaken to determine different parameters such as serum glucose, creatinine, urea, triglycerides, and cholesterol, compared with sialic acid because it is an acute phase indicator of inflammation as a risk factor for diabetes. BMI is also considered because being overweight or obese is mostly associated with diabetes due to disturbed carbohydrate metabolism.
In this study a total of 200 individuals of both genders were included which were divided into four groups including control (with no diabetes), diabetics (without complication), diabetics (with nephropathy complications) and diabetics with retinopathy. Each group comprising of 50 individuals subjected to estimation of serum sialic acid (SA), blood sugar, creatinine, urea, hemoglobin A1c (HbA1c), triglycerides and cholesterol as milligram per deciliter with body mass index (BMI). Blood (5 ml) was collected from anti cubital veins in sterile syringes after 12 h fasting from all individuals of each group. The blood for HbA1c was separated in vial having ethylenediaminetetraacetic acid (EDTA). The samples were collected from different hospitals and educated families after getting written consent from each person and results were kept confidential with fictitious numbers. The basal metabolic index was also calculated.
The individuals were mixed male, females from 25 to 55 years having diabetes for the last 10 to 12 years and were under medication of one or the other type (tablet or insulin). The patients with cardiovascular diseases, cancer or kidney failure were excluded from the study. The serum was extracted by centrifugation at 2000 rpm and was stored at 4°C in the refrigerator until analyzed (Svennerholm, 1957). HbA1c, an indicator of degree of metabolic control of blood sugar was estimated using the spectrophotometry technique (Crook et al., 2001). The HbA1c kit was supplied by Seimens Company (Hoelzel et al., 2004). The BMI was calculated using formula weight in kg/height in m2 (Katia et al., 2015). The other risk factor parameters in the serum were also estimated by colorimetric method with spectrophotometer using enzymatic kits from Roche.
The data thus obtained was analyzed by SPSS version 18 to find out mean and standard deviation (mean SD). The BMI is represented as a range for each parameter in each group considering 24.9 as the normal BMI. No complicated case of retinopathy was included in the study and the diabetics with complaint of occasional blurred vision were taken as retinopathy group relying on their eye testing report and no gross retinal symptom was reported. All the data is presented in Table 1 and Figure 1. The study was conducted between May, 2011 and May, 2014 (sample collection took more time). The blood samples were analyzed at Biochemistry Laboratory, Institute of Molecular Biology, The University of Lahore, Andrology Laboratory, Fatima Memorial Hospital, Lahore, Ali Diagnostic Laboratory Ali Hospital Lahore and Biotechnology Laboratory GC University Faisalabad, Pakistan.
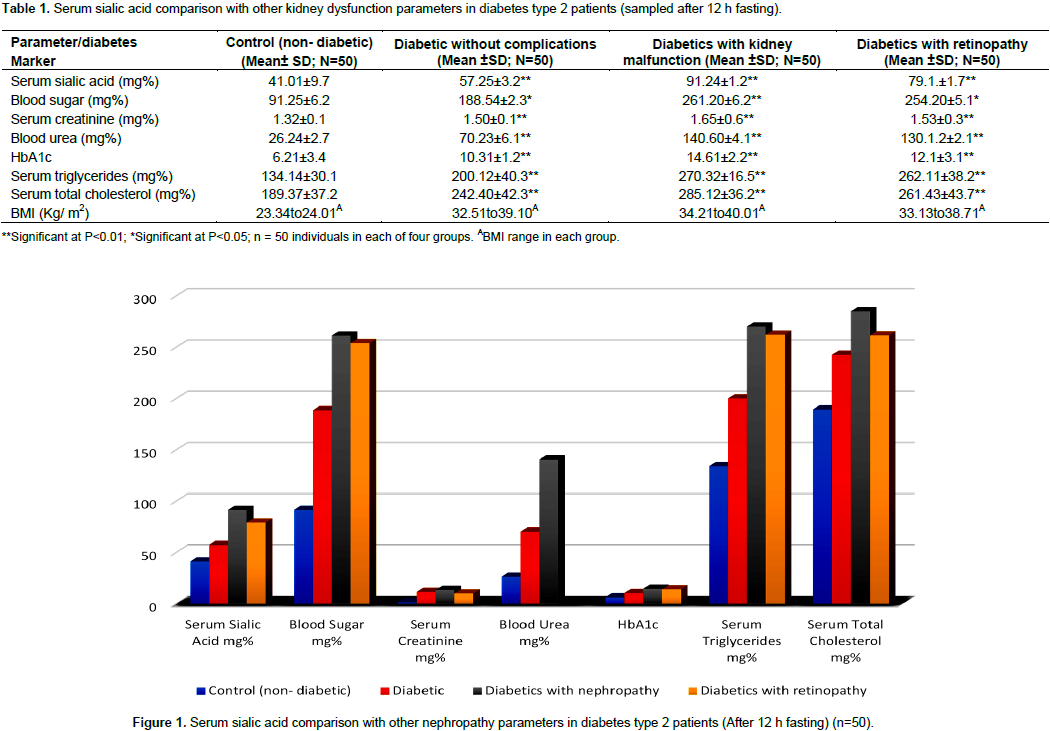
The serum sialic acid concentration in non-diabetics (Control) and diabetics with or without complications are given in Table 1 and Figure 1. In order to observe preference of sialic acid over the other risk factors such as serum sugar, serum creatinine, blood urea, serum triglycerides, serum total cholesterol, HbA1c and BMI; the mean ± standard deviation (SD) were compared with SA based on their serum levels in diabetes with control and between diabetic groups for their significance. In no subject was reported urine albumin, therefore, this parameter was not included. The control subjects showed 41.01 ± 9.7 mg% serum sialic acid as compared to 57.25 ± 3.2 mg% in diabetics with no complication, 91.24 ± 1.2 mg% in diabetics with nephropathy and 79.1 ± 1.7 mg% in diabetics with retinopathy and were compared statistically using mean ± SD. The BMI of controls was also compared with other three groups. 50 individuals irrespective of genders were selected in each group in this cross-sectional study. In all groups, the serum SA showed higher levels than control group which had values close to normal physiological levels.
The blood sugar also showed significantly higher levels in all the three diabetic groups as compared to the control group. The diabetics with nephropathy showed significantly higher (P<0.01) blood sugar levels, that is, 261.20 ± 6.2 and 254.20 ± 5.1 mg% in diabetics with retinopathy as compared to 188.54 ± 2.3 mg% in diabetics without complications. All subjects, except the control group, showed significantly higher blood sugar levels than 91.25 ± 6.2 mg% blood sugar. The serum creatinine also revealed significant differences as compared with the control which was 1.32±0.1 mg%, 1.5±0.1 mg% in diabetics without complications, 1.65±0.6 mg% in diabetics with complications and 1.53±0.3 mg% in diabetics with retinopathy, respectively. However, the diabetic groups did not show significant differences within diabetic groups but had significantly higher values than the control group.The blood urea was 26.24±2.7 mg% in the control group, 70.23±6.1 mg% in diabetics without complications, 140.60±4.1 mg% in diabetics with complications and 130.12± 2.1 mg% in diabetics with retinopathy.
The values for HbA1c also showed differences which had 6.21± 3.4 for control group, for diabetics without complications was 10.31±2.12, for diabetics with complications was 14.61± 2.2 and for diabetics with retinopathy was 12 .1± 3.1.Serum triglycerides revealed significant differences as 134.14±30.1 for control group, 200.12±40.3 mg% for diabetics without complications, 270.32±16.5 mg% for diabetics with complications and 262.11± 38.2 mg% for diabetics with retinopathy. The results for serum total cholesterol revealed major differences in the values that were, 189.37± 37.24 for control group, 242.40±42.3 mg% for diabetics without complications, 285.12± 36.2 mg% for diabetics with nephropathy and 261.43± 43.7 mg% for diabetics with retinopathy. The differences in serum values can be visualized at a glance in Figure 1.The values for BMI were estimated as range for each group which showed differences approaching over weight and obesity levels that were, 23.34 to 24.01 m2 for control group, 32.51 to 39.10 m2 for diabetics without complications, 34.21 to 40.01 m2 for diabetics with nephropathy and 33.13 to 38.71 m2 for diabetics with retinopathy.
Finding diabetic individuals for the study was a bit hard task but those who understood the research motive, gave consent without argument and many wanted results which were provided confidentially to desirous individuals. Most of the patients were only relying on blood and urine sugar tests with long intervals and continued treatment prescribed years back by a physician. Therefore the present results of their tests gave them a good guideline for treatment. The results presented in Table 1 and Figure 1 pertaining to different diabetic conditions may be helpful for further treatment of diabetes. The elevated serum sialic acid levels as compared to control subjects were indicative of diabetic complications. The serum SA within diabetic groups also showed significant differences. The results are in agreement with the findings of Shahid and Mehboob (2006) who conducted a similar study (Mahboob, 2008). These findings also correlate with the results presented by Crook (1993). The present findings in Table 1 and Figure 1 showed that serum SA can be trusted as indicator of diabetes.
The blood sugar level of diabetics with or without complications was significantly higher as compared to control group indicating the effect of diabetes on kidney function due to elevated levels of different parameters used for diabetes diagnosis. The findings are similar to the results presented by Linderberg et al. (1991). Almost parallel findings were reported for blood glucose level by Gavella et al. (2003) in different diabetic complications. These results indicate that diabetes has different effects on kidney function as the level of blood sugar increases therefore dietary control along with medication is equally important.The kidney function parameters such as serum creatinine and urea in diabetics were also higher in all diabetic groups as compared to control group. However, the serum creatinine in diabetics without complications, diabetics with complications and diabetics with retinopathy did not show significant differences yet the creatinine level had entered critical threshold than can be accommodated by nephrons. Similarly urea was a few times higher in diabetics as compared to control group which indicates the protein metabolism disturbances and needs specific management.
HbA1c is an indicator of kidney ability to handle glucose and the damage done to kidney was compared in all three diabetic groups. The HbA1c level was significantly higher than control group showing the damage so far done to kidney cells for handling serum glucose. These findings match with the results reported by Nayak and Bhakhta (2005) who conducted a similar study. Similar results were reported by Svennerholm (1957) indicating diabetic damage on kidney. Similarly the serum triglycerides and total cholesterol concentration was higher in diabetics as compared to control group. The triglycerides and cholesterol also indicate cardiovascular diseases along with diabetes. At the same time higher levels of TG and cholesterol may also be hazardous for kidney function and indicate several other complications in addition to diabetes. These findings are similar to the findings of Jeremy (2003) and WHO (1985).
The triglycerides and cholesterol are alarming indicators for hypertension and cardiovascular diseases in addition to adverse effect on kidney function. Similar findings on TG and cholesterol were reported by Pickup et al. (1997). This shows that elevated serum sugar is closely associated with other metabolites creating a risk for cardiovascular and renal normal functioning. The basal metabolic index (BMI) is closely related with body mass, body fat and body weight (Table 1). It is evident that BMI in all the three diabetic groups was higher than control group but between diabetic groups, the BMI was not grossly different. The results in Table 1 show that BMI ranges of diabetic groups were even higher than the overweight level which is very alarming signal for several diseases including hypertension, diabetes and cardiovascular diseases.
From the results presented in Table 1 and Figure 1, that serum SA is very closely related with different diabetic conditions including nephropathy or retinopathy. However the glycemic control indicated by blood sugar and HbA1c and the renal functioning threshold estimated by serum urea, creatinine contents along with body mass index all go together in damaging kidneys if not controlled. It is suggested that all the parameters discussed are of similar importance for diabetic control and treatment. It may be inferred that serum SA is more closely related with diabetic complications than other parameters which show acute stage and also has relationship with cardio-vascular diseases. Therefore, elevated level of serum SA may be taken as an important indicator of diabetic nephropathy.
The authors have not declared any conflict of interests.
The authors are grateful to the Ali Hospital’s Administration, Head of Bio Technology Department GCU, Faisalabad and FMH Diagnostic Laboratory for allowing sample analysis using their equipment.
REFERENCES
|
Chen JW, Gall MA, Yokoyama H, Jensen JS, Deckert M, Parving HH (1996). Raised serum sialic acid concentration in NIDDM patients with and without diabetic nephropathy. Diabetes Care 19(2):130-134.
Crossref
|
|
|
|
Cohen JD, Grimm RH, Smith WM (1981). Multiple risk factor intervention trial (MRFIT): VI. Intervention on blood pressure. Prev. Med. 10(4):501-518.
Crossref
|
|
|
|
|
Crook M (1993). The determination of plasma or serum sialic acid. Clin. Biochem. 26(1):31-38.
Crossref
|
|
|
|
|
Crook MA, Pickup JC, Lumb PJ, Georgino F, Webb DJ, Fuller JH (2001). Relationship between plasma sialic acid concentration and microvascular and macrovascular complications in type 1 diabetes. Diabetes Care 24(2):316-322.
Crossref
|
|
|
|
|
Gavella M, Lipovac V, Car A, VuÄić M, Sokolić L, Rakoš R (2003). Serum sialic acid in subjects with impaired glucose tolerance and in newly diagnosed type 2 diabetic patients. Acta Diabetol. 40(2):95-100.
|
|
|
|
|
Ghosh J, Datta S, Pal M (2016). Role of sialic acid in prediction of diabetic nephropathy. Al Ameen J. Med. Sci. 9(1):58-64.
|
|
|
|
|
Guyton C, Hall JE (2016). Text Book of Medical Physiology. 13th Ed. Elsevier.
|
|
|
|
|
Hoelzel W, Weykamp C, Jeppsson JO, Miedema K, Barr JR, Goodall I, Hoshino T, John WG, Kobold U, Little R, Mosca A (2004). IFCC reference system for measurement of hemoglobin A1c in human blood and the national standardization schemes in the United States, Japan, and Sweden: a method-comparison study. Clin. Chem. 50(1):166-174.
Crossref
|
|
|
|
|
Jeremy WT (2003). Treating hypertension in diabetic nephropathy. Diabetes Care 26:180-205.
|
|
|
|
|
Katia LR, Abreu AAM, Marquez CG, Stanescu RL, Martin MIM, Fernandez EP (2015). Diabetic Nephropathy without Diabetes. J. Clin. Med. 4(7):1403-1427.
Crossref
|
|
|
|
|
Lindberg G, Eklund GA, Gullberg B, Råstam L (1991). Serum sialic acid concentration and cardiovascular mortality. BMJ 302(6769):143-146.
Crossref
|
|
|
|
|
Mahboob SMST (2008). Electrolytes and Na-K-ATPase: potential risk factors for the development of diabetic nephropathy. Pak. J. Pharm. Sci. 21(2):172-179.
|
|
|
|
|
Mehta SR, Kashyap AS, Das S (2009). Diabetes mellitus in India: The modern scourge. Med. J. Armed Forces India 65(1):50-54.
Crossref
|
|
|
|
|
Nayak BS, Bhakhta G (2005). Relationship between Sialic acid and metabolic variables in Indian type 2 diabetic patients. Lipid Health Dis. 4(1):15
Crossref
|
|
|
|
|
Pickup JC, Mattock MB, Chusney GD, Burt D (1997). NIDDM as a disease of the innate immune system: association of acute-phase reactants and interleukin-6 with metabolic syndrome X. Diabetologia 40(11):1286-1292.
Crossref
|
|
|
|
|
Pradhan AD, Manson JE, Rifai N, Buring JE, Ridker PM (2001). C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 286(3):327-334.
Crossref
|
|
|
|
|
Salhanick AI, Amatruda JM (1988). Role of sialic acid in insulin action and the insulin resistance of diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 255(2):E173-E179.
Crossref
|
|
|
|
|
Shahid SM, Mahboob T (2006). Clinical correlation between frequent risk factors of diabetic nephropathy and serum sialic acid. Int. J. Diabetes Metab. 14:138-144.
|
|
|
|
|
Svennerholm L (1957). Quantitive estimation of sialic acids: II. A colorimetric resorcinol-hydrochloric acid method. Biochim. Biophys. Acta 24:604-611.
Crossref
|
|
|
|
|
WHO-World Health Organization (1985). Diabetes Mellitus, Report of a WHO study group, Geneva, Switzerland: World Health Organization.
|
|
|
|
|
Yarema K (2006). The sialic acid pathway in human cells. Baltimore: John Hopkins University, pp. 149-152.
|
|