Full Length Research Paper

ABSTRACT
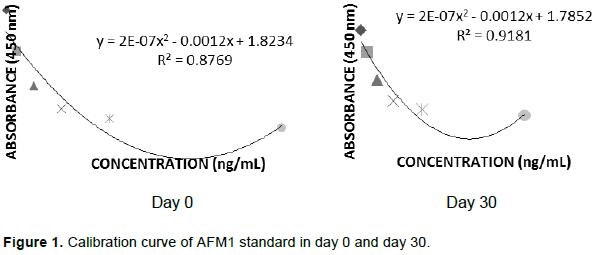
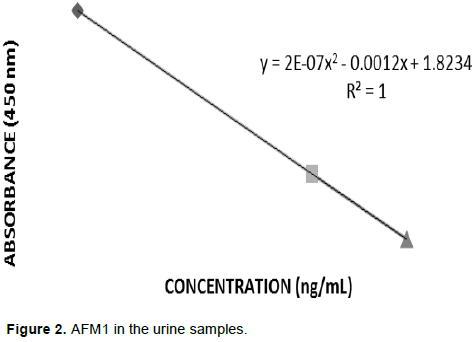
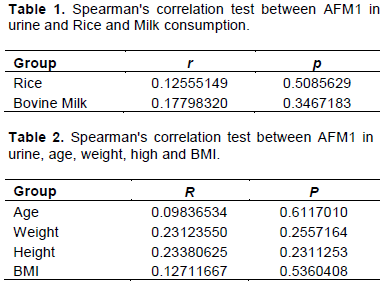
Aflatoxins are the main mycotoxin related to the contamination of Brazil nut and an important product extracted from the Amazon region that has a high number of consumers due to its health benefits. Considering the frequent occurrence of aflatoxins in Brazil nuts, it is necessary to study the levels of exposure to these toxins associated with its consumption using biomarkers. To do this, a study was carried out with 30 volunteers of both sexes, where each volunteer received a kit containing Brazil nuts for the ingestion of 2 (two) units / day for 30 days. Urine samples were collected from each volunteer at 0 and 30 days, and the level of Aflatoxin M1 (AFM1) was determined by ELISA using the Helica Kit®. A questionnaire was used to obtain information on weight, height, age, medication use, pathological conditions, frequency of weekly consumption of certain foods more susceptible to aflatoxin contamination, and 24-h food recall. Of the 30 samples analyzed at time 0 (zero) for exposure, AFM1 presented positive results in 3 (10%) samples with a range of 2.75-70.41 ng/mL. In the analysis of the 30 days after Brazil nut consumption, the presence of AFM1 in the urine was not detected, suggesting that Brazil nut consumption did not generate impact on the urinary levels and exposure to AFM1. In conclusion, no association was found between food consumption of food susceptible to aflatoxin contamination and concentration of AFM1 in urine.
Key words: Aflatoxin, nuts, ELISA, selenium.
INTRODUCTION
MATERIALS AND METHODS
RESULTS AND DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
REFERENCES
|
Ali N, Blaskewicz M, Hossain K, Degen GH (2017). Determination of aflatoxin M1 in urine samples indicates frequent dietary exposure to aflatoxin B1 in the Bangladeshi population. International Journal of Hygiene and Environmental Health 220:271-281. |
|
|
Bando E, Gonçales LN, Tamura NK, Machinski Junior M (2007). Biomarkers for assessment of human exposure to mycotoxins. Jornal Brasileiro de Patologia e Medicina Laboratorial 43:175-180. |
|
|
Baquião AC, Zorzete P, Reis, TA, Assunção E, Vergueiro S, Correa B (2012). Mycoflora and myotoxins in Field samples of Brazil nuts. Food Control 28:224-229. |
|
|
Beltran E, Ibanez M, Sancho JV, Cortes MA, Yusa V, Hernandez F (2011). UPLC-MS/MS highly sensitive determination of aflatoxins, the aflatoxin metabolite M1 and ochratoxin A in baby food and milk. Food Chemistry 126:737-744. |
|
|
Becker-Algeri TA, Castagnaro D, de Bortoli K, De Souza C, Drunkler DA, Badiaçle-Furlong E (2016). Mycotoxins in Bovine Milk and Dairy Products: A Review. Journal of Food Science 81(3):R544-5552. |
|
|
Benkerroum N (2019). Retrospective and Prospective Look at Aflatoxin Research and Development from a Practical Standpoint. International Journal of Environmental Research and Public Health 16:363. |
|
|
Bui-Klimke TR, Wu F (2015). Ochratoxin A and human health risk: A review of the evidence. Critical Reviews in Food Science and Nutrition 55(13):1860-1869. |
|
|
Chen C, Mitchell, NJ, Gratz J, Houpt ER, Gong Y, Egner PA, Groopman JD, Riley RT, Showker JL, Svensen E, Mduma ER, Patil CL, Wu F (2018). Exposure to aflatoxin and fumonisin in children at risk for growth impairment in rural Tanzania. Environment International 115:29-37. |
|
|
European Food Safety Authority (EFSA) (2005). Opinion of the Scientific Committee on a request from EFSA related to a harmonized approach for risk assessment of substances which are both genotoxic and carcinogenic [Internet]. EFSA Journal. |
|
|
Fay MP, Proschan MA (2010). Wilcoxon-Mann-Whitney or t-test? On assumptions for hypothesis tests and multiple interpretations of decision rules. Statistics Surveys, Institute of Mathematical Statistics 4:1-39. |
|
|
Genest C, Neslehova JG, Remillard B (2013). On the estimation of Spearman's rho and related tests of independence for possibly discontinuous multivariate data. Journal of Multivariate Analysis 117: 214-228. |
|
|
He Y, Fang J, Peng X, Cui H, Zuo Z, Deng J, Chen Z, Geng Y, Lail W, Hatch MC, Chen CJ, Levin B, Ji BT, Yang GY, Hsu SW, Wang LW, Hsieh LL, Santella RM (1993a). Urinary aflatoxin levels, hepatitisâ€B virus infection and hepatocellular carcinoma in Taiwan. International Journal of Cancer 54(6):931-934. |
|
|
Hatch MC, Chen CJ, Levin B (1993b). Urinary aflatoxin levels, hepatitis-B virus infection and hepatocellular carcinoma in Taiwan. International Journal of Cancer 54:931-934. |
|
|
Heshmati A, Milani JM (2010). Contamination of UHT milk by aflatoxin M1 in Iran. Food Control 21:19-22. |
|
|
International Agency for Research on Cancer (IARC) (1993). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, v. 56. Some Naturally Occurring Substances: Food Items and Constituents, Heterocyclic Aromatic Amines and Mycotoxins. IARC Press, Lyon. |
|
|
Institute of Medicine (IOM) (2001). Food Safety Policy, Science, and Risk Assessment: Strengthening the Connection. Workshop Proceedings. Food Forum, Food and Nutrition Board. National Academy Press, Washington, DC. |
|
|
Jardim ANO, Caldas E (2009) Chemical Dietary Exposure and the risks to human health. Quim. Nova 32(7):1898-1909. |
|
|
Jager AV, Tonin FG, Baptista GZ, Souto RT, Oliveira CAF (2016). Assessment of aflatoxin exposure using serum and urinary biomarkers in São Paulo, Brazil: A pilot study. International Journal of Hygiene and Environmental Health 219(3):294-300. |
|
|
Jager AV, Tonin FG, Baptista GZ, Souto RT, Oliveira CAF (2014). Determination of Urinary Biomarkers for Assessment of Short-Term Human Exposure to Aflatoxins in São Paulo, Brazil. Toxins 6:1996-2007. |
|
|
Jonsyn-Ellis FE (2000). Seasonal variation in exposure frequency and concentration levels of aflatoxin and ochratoxins in urine samples of boys and girls. Mycopathologia 152:35-40. |
|
|
Kruschke JK (2014). Doing Bayesian data analysis: A tutorial with R, JAGS, and Stan. 2. ed. Londres: Academic. |
|
|
Leong Y, Rosmab A, Aishah A, Latiff A, Izzah N (2012). Associations of serum aflatoxin B1-lysine adduct level with socio-demographic factors and aflatoxins intake from nuts and related nut products in Malaysia. International Journal of Hygiene and Environmental Health 215:368-372. |
|
|
Limaye A, Yu R, Chou C, Liu J, Cheng K (2018). Protective and Detoxifying Effects Conferred by Dietary Selenium and Curcumin against AFB1-Mediated Toxicity in Livestock: A Review. Toxins 10:25. |
|
|
Majeed S, De Boevre M, De Saeger S, Rauf W, Tawab A, Habib F, Rahman M, Iqbal, M (2018). Multiple Mycotoxins in Rice: Occurrence and Health Risk Assessment in Children and Adults of Punjab, Pakistan. Toxins 10(2):77. |
|
|
Moreira MF, Oliveira TR, Vieira IGP, Freire FCO, Silva SC, Ribeiro LM (2016). Occurrence of fungi and aflatoxins B in nuts and products marketed the Brazilian northeastern regions. Revista do Instituto Adolfo Lutz 75:1698. |
|
|
Nugraha A, Khotimah K, Rietjens IMCM (2018). Risk assessment of aflatoxin B1 exposure from maize and peanut consumption in Indonesia using the margin of exposure and liver cancer risk estimation approaches. Food and Chemical Toxicology 113:134-144. |
|
|
Pacheco AM, Scussel VM (2009). Aflatoxins evaluation on in-shell and shelled dry Brazil nuts for export analyzed by LC-MS/MS-2006 and 2007 harvests. World Mycotoxin Journal 2:295-304. |
|
|
Qian GS, Ross RK, Yu MC, Yuan JM, Gao YT, Henderson BE, Wogan GN, Groopman JD (1994). A follow-up study of urinary markers of aflatoxin exposure and liver cancer risk in Shanghai, People's Republic of China. Cancer Epidemiology, Biomarkers and Prevention 3:3-10. |
|
|
Redzwan SM, Rosita J, Sokhini AMM, Aquilah ARN (2012). Association Between Aflatoxin M1 Excreted in Human Urine Samples with the Consumption of Milk and Dairy Products. Bulletin of Environmental Contamination and Toxicology 89(6):1115-1119. |
|
|
Reis TA, Oliveira TD, Baquião AC, Gonçalves SS, Zorzete P, Correa B (2012). Mycobiota and mycotoxins in Brazil nut samples from different states of the Brazilian Amazon region. International Journal of Food Microbiology 159:61-68. |
|
|
Romero CA, Ferreira TRB, Dos Santos Dias CT, Calori-Domingues MA, Da Gloria E M (2010). Occurrence of AFM1 in urine samples of a Brazilian population and association with food consumption. Food Control 21:554-558. |
|
|
Schleicher RL, McCoy LF, Powers CD, Sternberg MR, Pfeiffer CM (2013). Serim concentrations of an aflatoxin-albumin adduct in the National Health and Nutrition Examination Survey (NHANES) 1999-2000. Clinica Chimica Acta 423:46-50. |
|
|
Strunz CC, Oliveira TV, Vinagre JC, Lima A, Cozzolino S, Maranhao RC (2008). Brazil nut ingestion increased plasma selenium but had minimal effects on lipids, apolipoproteins, and high-density lipoprotein function in human subjects. Nutrition Research 28(3):151-155. |
|
|
Thomson CD, Chisholm A, McLachlan SK, Campbell JM (2008) Brazil nuts: an effective way to improve selenium status. The American Journal of Clinical Nutrition 87(2):379-84. |
|
|
Vargas EA, Santos EA, Whitaker TB, Slate AB (2011). Determination of aflatoxin risk components for in-shell Brazil nuts. Food Additives and Contaminants Part A 28:1242-1260. |
|
|
Zhu JQ, Zhang LS, Hu X, Xiao Y, Chen, JS, Xu YC, Fremy J, Chu FS (1987). Correlation of dietary aflatoxin B1 levels with excretion of aflatoxin M1 in human urine. Cancer Research 47:1848-1852. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


