Full Length Research Paper

ABSTRACT
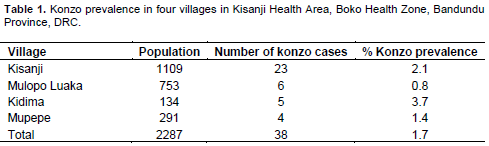
Persistent konzo is low level incidence of konzo that is not associated with konzo epidemics due to drought or war. It has been reported from Mozambique and Tanzania. Various health factors associated with persistent konzo in four villages in Kasanji Health Area, Bandundu Province, DRC were studied, where there were 38 konzo cases in a population of 2283, with mean percentage konzo prevalence of 1.7%. Konzo occurred over the years since 1951 with 0 to 3 cases per year. Anthropometric measurements of children aged 0.5 to 14 y showed that 47% were stunted, 24% underweight, 16% had chronic energy deficiency and 16 to 24% suffered malnutrition. There was no significant difference between children from konzo households or from non-konzo households. The % konzo prevalence (%K) calculated from the equation %K = 0.06 %T + 0.035 %M, where %T = percentage of school children with urinary thiocyanate levels >350 µmol/L and %M = percentage of malnutrition, gave %K = 1.6 from non-konzo households and %K = 2.2 from konzo households, which agrees with the actual mean value of 1.7. However, the equation does not apply when either %T or %M is zero or for very high values of %K > 9.5. The value of %K is nearly twice as sensitive to changes in %T as to changes in %M, which partly explains the greater ease of prevention of konzo by reducing %T to zero, using the wetting method to remove cyanogens from cassava flour, than by reducing %M by broad based methods.
Key words: Konzo prevalence, malnutrition, school children, urinary thiocyanate, cassava cyanide.
INTRODUCTION
Konzo is a spastic paraparesis that causes irreversible paralysis of the legs mainly in children and young women, associated with intake of large amounts of cyanide from a diet of bitter cassava that also causes malnutrition (Cliff et al., 1985; Howlett et al., 1990; Nzwalo and Cliff, 2011). It is worst in the Democratic Republic of Congo (DRC), also occurs in Mozambique, Tanzania, Cameroon, Central African Republic, Angola and there are reports of its recent spread to Uganda (Diasolua-Ngudi, 2015) and Zambia (Mbewe, 2015). The condition was first described by Trolli (1938) working in the Belgian Congo (now DRC) and it has persisted there up to the present time. Konzo occurs most commonly during the time of the cassava harvest when cassava intake is at a maximum. A study developed a simple equation that relates the % konzo prevalence (%K), with the % malnutrition (%M) calculated from a food consumption survey and the percentage of children with high urinary thiocyanate content (%T), (determined near the time of cassava harvest), which is a good estimate of their cyanide intake (Banea et al., 2015a).
Konzo epidemics occur due to drought when water-stressed cassava plants make 2 to 4 times as much cyanogenic glucoside as normal (Bokanga et al., 1994), and the increased level of cyanide is transferred to the processed cassava flour (Cardoso et al., 2005), which causes cyanide poisoning and konzo (Cliff et al., 2011). Konzo epidemics also result from war when local village people are forced from their homes and gardens and forced to eat unprocessed high cyanide cassava from the bush (Cliff et al., 1997; Nhassico et al., 2008; Chabwine et al., 2011). Konzo outbreaks also occur in Central Africa when peeled cassava roots are not immersed in water for the 3 to 4 days necessary to allow the enzyme linamarase to break down fully the cyanogenic glucoside, but are short soaked for only 1 to 2 days. (Banea et al., 1992). By contrast, konzo can occur at a low level of about one per village per year called persistent konzo, and has been observed in Mozambique (Ernesto et al., 2002) and Tanzania (Howlett, 1994).
The study reports on four villages in the DRC, in which persistent konzo has occurred over many years and various health factors such as the degree of malnutrition, stunting and high cyanide intake from cassava that together are associated with persistent konzo.
MATERIALS AND METHODS
A population census was carried out. People with walking difficulties were examined for konzo following the criteria established by World Health Organisation (WHO, 1996): a spastic visible walk or run, a history of sudden onset within a week of a person in good health, bilateral exagerration of knee jerks and/or Achillian reflexes and non-progressive evolution of the disease. In each household with a case of konzo, the study identified the nearest household with no case of konzo (control household). Anthropometric measurements of weight and height were made on 24 to 31 children aged 6 to 59 months and of 31 children aged 5 to 14 years from konzo households and about 50 children from non-konzo control households. Height for age was recorded and children whose height for age was below minus two standard deviations from the median of WHO standards of child growth were classified as stunted. The weight for age was calculated and those whose weight for age was below minus two standard deviations from the median weight for age of the WHO reference population were classified as underweight. The body mass index (BMI) was calculated by dividing the weight (kg) by the square of the height in metres and those whose BMI for age was below minus two standard deviations from the median BMI for age were considered to have chronic energy deficiency.
Study area and agriculture
The survey was conducted in four villages; Kasanji, Mulopo Luaka, Kidima and Mupepe of Kasanji Health Area in Boko Health Zone on August 21 to 29, 2014 (Banea et al., 2015a). The villages are in the savanna and the main crops are cassava, maize and groundnuts, which are also cash crops. The rainy season extends from October to April and the dry season from May to September. There are major conflicts of succession of leaders and land disputes between several families.
Food consumption survey, food consumption score (FCS) and percent malnutrition (%M)
The number of days in which different foods were eaten during the week preceding the survey was obtained by a survey of 31 konzo and 31 non-konzo households. The food consumption score (FCS) was calculated and interpreted using the methods of the World Food Program (Interagency Workshop Report WFP-FAO, 2008; Banea et al., 2015a). The percentage malnutrition (% M) was calculated (Banea et al., 2015b) for konzo and non-konzo control households. The socio-economic conditions of konzo households and non-konzo households was also compared with respect to type of roof, whether straw or sheet metal on houses, toilet facilities, furniture and other effects within houses.
Urinary thiocyanate analysis, calculation of %T and %K
Urine samples were obtained from 41 school children aged 5 to 14 y in konzo households and 63 school children from non-konzo control families, with oral consent of their parents. These samples were obtained from Kasanji 60, Mulopo Luaka 18, Kidima 19 and Mupepe 7, and were analysed on site using the simple picrate thiocyanate kit D1, http://biology.anu.edu.au/hosted_sites/CCDN/; Haque and Bradbury, 1999). A colour chart with ten shades of colour from yellow to brown was used, which corresponded to 0 to 1720 µmol thiocyanate/L. The percentage of children with urinary thiocyanate levels >350 µmol/ (%T) was calculated for konzo and non-konzo control families. The % konzo prevalence was calculated by the equation % K = 0.06 %T + 0.035 %M (Banea et al., 2015a).
RESULTS
In the four villages there were 47 persons with walking difficulties which included 38 konzo cases with a mean konzo prevalence of 1.7% (Table 1). Detailed examination of konzo cases showed that all had an abrupt beginning of 1 to 7 days, with 82% beginning in one day. The knee jerks bilateral occurred in 92% of cases and Achilles reflexes in 60% of cases. With regard to walking, 84% were mildly disabled not using a stick to walk and 16% were moderately disabled requiring one or two sticks to walk. Speech disorders occurred with 68% of patients and 45% had impaired vision. Of the konzo cases, 63% were women, 37% men; 37% were single, 61% married and 2% widowed. Half of the patients had at least one relative dead or alive with konzo.
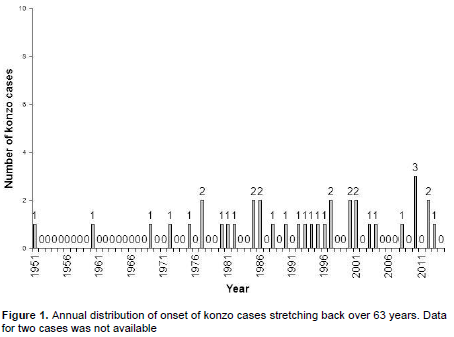
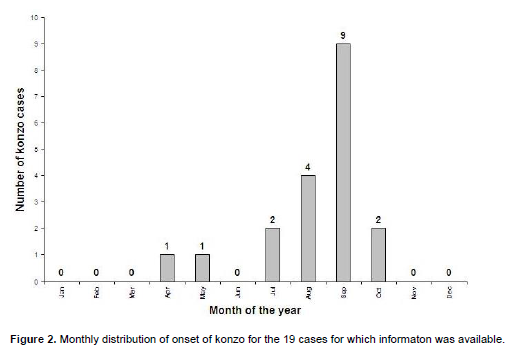
The distribution of onset of konzo over the years is shown in Figure 1, two persons did not remember the year of onset. Only 19 people recalled the exact month of onset of konzo and this data is shown in Figure 2. About 80% of the houses had straw roofs which leaked water in the wet season, nearly all households had unimproved toilets, all households used improved water sources for drinking water, but this involved a 30 min walk. Nearly all houses had chairs and tables, 60% had a radio, 35% a shotgun and two thirds of those from non-konzo households had a telephone compared with only one third from a konzo household.
Anthropometric measurements made on children aged 6 to 59 months from 24 konzo households and 47 non-konzo households showed that 47% were stunted and 24% underweight with no significant differences between those from konzo or non-konzo households. For 31 school children aged 5 to 14 years from konzo households and 53 from non-konzo households the stunting was virtually the same at 48% as from children aged 6 to 59 month. Furthermore, 16% of school children had BMI for age below minus two standard deviations from the median BMI for age, called chronic energy deficiency. There was no significant difference between the % stunting or the % chronic energy deficiency for those children 5 to 14 years from konzo or non-konzo households.
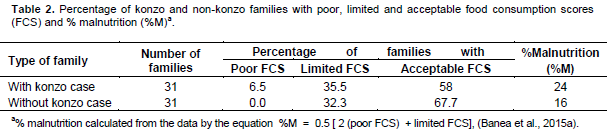
The results of the food consumption survey of 31 konzo households and 31 non-konzo households is given in Table 2, together with the percentage malnutrition (%M) calculated for the konzo and non-konzo households. In Table 3 is shown the percentage of school children with >350 µmol/L urinary thiocyanate levels (%T) from konzo and non-konzo households and also the % konzo prevalence (%K) calculated from the data for %T (Table 3) and %M (Table 2).

DISCUSSION
Persistent konzo, also sometimes known as endemic or sporadic konzo, occurs at the rate of one or two konzo cases per village per year. It has been previously observed in Mozambique (Ernesto et al., 2002) and Tanzania (Howlett, 1994). The distribution of konzo in these four villages over the years since 1951 is shown in Figure 1 and there are small or zero numbers of konzo cases each year, rather than the variable and increasing numbers found in recent years in our other studies (Banea et al., 2013, 2015b). Lest it is thought that these cases of persistent konzo only amount to a very few cases compared to the many cases that occur during an epidemic due to drought, war or short soaking and it should be noted that a recent survey of thirty villages in Kwilu District of Bandundu Province in which there were 26 villages with low konzo prevalence of 0.11 to 1.1%, accounted for 58% of the total 172 konzo cases (Banea et al., 2015b). It is therefore important to consider persis-tent konzo where cases are spread thinly over a large number of villages, thus affecting large numbers of people.
The monthly distribution of onset of 19 of the konzo cases who could remember the month of onset is shown in Figure 2. The peak konzo onset (September) also corresponds with the time of the cassava harvest when cassava consumption peaks, as has been found in virtually every study on konzo. This corresponded with the time of late August for the visit by the study group, which is also the time when the percentage of school children with high urinary thiocyanate (>350µmol/L) levels should be measured (Banea et al., 2015a). The study was designed to show up differences between konzo households and non-konzo households in the same village but no significant differences were observed, except that the ownership of telephones was twice as great in non-konzo households compared with konzo households. Similarly, it has been difficult to establish differences between the urinary thiocyanate levels of school children with konzo and those without konzo, but one study has shown a significant increase amongst konzo children compared with non-konzo children carried out at the time of the cassava harvest (Banea et al., 2013).
An anthropometric study of 500 children aged 0 to 36 months in a non-konzo area north of the Kasai river and of a konzo area south of the river in Bandundu Province, DRC, showed that the height for age index was significantly lower in children from the southern konzo area (indicative of stunting), but there was no significant differences in weight for height or weight for age indices (Banea et al., 2000). In konzo villages, the level of stunting is about 40% amongst children less than 5 years old (Diasolua-Ngudi, 2015). In these four villages with persistent konzo, the study found 47% of the children aged 0.5 to 14 years were stunted, which agrees with Diasolua-Ngudi (2015). In addition, 24% were underweight and 16% suffered from chronic energy deficiency. The food consumption survey (Table 2) showed that 16 to 24% of the population had malnutrition.
Calculation of % konzo prevalence (%K)
The urinary thiocyanate data from 104 school children from konzo and non-konzo households in Table 3 records the percentage of school children with high urinary thiocyanate content (%T). This is used in equation (1) to calculate %K expected with konzo households (2.2%) and with non-konzo households (1.6%). The actual mean value of %K for the four villages is 1.7% (Table 1). The good agreement between the actual mean value of %K and the calculated value from Equation (1) shows that this simple empirical equation is useful. However, the equation does not apply if either %M or %T is zero (Banea et al., 2015a) or above the upper range of the equation, when %K > 9.5. Recently, Banea et al. (2015b) found in Kongila Ndola village in Kwilu District of DRC a very high konzo prevalence of 17%, perhaps due to very high cyanide intake by the school children which would produce very high urinary thiocyanate levels.
In Equation 1, it is noted that the value of %K is nearly twice as sensitive to a change in %T as it is to an equal change in %M.
CONCLUSION
The study report shows that %K can be reduced by twice the amount by reducing %T as it can by an equal reduction in %M. This is one reason why it is simpler and more effective to prevent konzo by reducing cyanide intake using the wetting method (Banea et al., 2014b, 2015a) rather than by improving the overall nutrition of village people (Kasongo and Calo, 2011; Delhourne et al., 2012). Indeed once %T is reduced to zero, by daily use of the wetting method by village women that removes cyanogens from the cassava flour, then konzo is prevented (Bradbury et al., 2015). Furthermore, the wetting method is much more direct in its application than a broad based holistic method (Delhourne et al., 2012).
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The author’s sincere thanks go to the village people, the chiefs of the villages and the health area medical doctor for their collaboration.
REFERENCES
|
Banea JP, Bradbury JH, Mandombi C, Nahimana D, Denton IC, Kuwa N, Tshala Katumbay D (2013). Control of konzo by detoxification of cassava flour in three villages in the Democratic Republic of Congo. Food Chem. Toxicol. 60:506-513. |
|
|
Banea JP, Bradbury JH, Mandombi C, Nahimana D, Denton IC, Foster MP, Kuwa N, Tshala Katumbay D (2015a). Konzo prevention in six villages in the DRC and the dependence of konzo prevalence on cyanide intake and malnutrition. Toxicol. Rep. 2:609-616. |
|
|
Banea JP, Bradbury JH, Mandombi C, Nahimana D, Denton IC, Kuwa N, Tshala Katumbay D (2014b). Effectiveness of wetting method for control of konzo and reduction of cyanide poisoning by removal of cyanogens from cassava flour. Food Nutr. Bull. 35:28-32. |
|
|
Banea JP, Bradbury JH, Nahimana D, Denton IC, Mashukano N, Kuwa N (2015b). Survey of the konzo prevalence of village people and their nutrition in Kwilu District, Bandundu Province, DRC. Afr. J. Food Sci. 9:43-50. |
|
|
Banea M, Poulter NH, Rosling H (1992). Shortcuts in cassava processing and risk of dietary cyanide exposure in Zaire. Food Nutr. Bull. 14:137-143. |
|
|
Banea-Mayambu JP, Tylleskar T, Tylleskar K, Gebre-Medhim M, Rosling H (2000). Dietary cyanide from insufficiently processed cassava and growth retardation in children in the Democratic Republic of Congo (formerly Zaire). Ann. Trop. Ped. 20:34-40. |
|
|
Bokanga M, Ekanayake IJ, Dixon AGO, Porto MCM (1994). Genotype environment interactions for cyanogenic potential in cassava. Acta Hortic. 375:131-139. |
|
|
Bradbury JH, Banea JP, Mandombi C, Nahimana D, Denton IC, Kuwa N 2015). Practical pointers for prevention of konzo in tropical Africa. (Field Exchange 50:62. Cardoso AP, Mirione E, Ernesto M, Massaza F, Cliff J, Haque MR, Bradbury JH (2005). Processing of cassava roots to remove cyanogens. J. Food Comp. Anal. 18:451-460. |
|
|
Chabwine JN, Masheka C, Balol'ebwami Z, Maheshe B, Balegamire S, Rutega B, wa Lola M, Mutendela K, Bonnet MJ, Shangalume O, Balegasmire JM, Nemery B (2011). Appearance of konzo in South Kivu, a wartorn area in the Democratic Republic of Congo. Food Chem. Toxicol. 40:644-649. |
|
|
Cliff J, Martensson J, Lundquist P, Rosling H, Sorbo B (1985). Association of high cyanide and low sulphur intake in cassava induced spastic paraparesis. Lancet 11:1211-13. |
|
|
Cliff J, Muquingue H, Nhassico D, Nzwalo H, Bradbury JH (2011). Konzo and continuing cyanide intoxication from cassava in Mozambique. J. Chem. Toxicol. 49:631-635. |
|
|
Cliff J, Nicala D, Saute F, Givragy R, Azambuja G, Taela A, Chavane L, Howarth J (1997). Konzo associated with war in Mozambique. Trop. Med. Int. Health 2:1068-1074. |
|
|
Delhourne M, Mayans J, Calo M, Guyot-Bender C (2012). Impact of cross-sectoral approach to addressing konzo in DRC. Field Exchange No. 44:50-54. |
|
|
Diasolua-Ngudi D (2015). 1000 days to prevent stunting among children in konzo affected areas. CCDN News, No. 25:10-11. |
|
|
Ernesto M, Cardoso AP, Nicala D, Mirione E, Massaza F, Cliff J, Haque MR, Bradbury JH (2002). Persistent konzo and cyanogen toxicity from cassava in northern Moxambique. Acta Trop. 82:357-362. |
|
|
Haque MR, Bradbury JH (1999). Simple method for determination of thiocyanate in urine. Clin. Chem. 45:1459-1464. |
|
|
Howlett WP (1994). Konzo: A new human disease entity. Acta Trop. 375:323-329. |
|
|
Howlett WP, Brubaker GR, Mlingi N, Rosling H (1990). Konzo, an epidemic upper motor neuron disease studied in Tanzania. Brain 113:223-235. |
|
|
Interagency Workshop Report WFP-FAO (2008). Measures of Food Consumption–Harmonizing Methodologies. April 2008, Rome. Italy. |
|
|
Kasongo E, Calo M (2011). A cross-sectoral approach to addressing konzo in DRC. Field Exchange, No 41:3-5. |
|
|
Mbewe RK (2015). Konzo disease breaks out in Mongu's Kaote village. |
|
|
Nhassico D, Muquingue H, Cliff J, Cumbana A, Bradbury JH (2008). Rising African cassava production, diseases due to high cyanide intake and control measures. J. Sci. Food Agric. 88:2043-2049. |
|
|
Nzwalo H, Cliff J (2011). Konzo: from poverty, cassava and cyanogen intake to toxico-nutritional neurological disease. PloS Negl. Trop. Dis. 5(6):e1051. |
|
|
Trolli G (1938). Paraplegie spastique epidemique, "Konzo" des indigenes du Kwango, In: G. Trolli, Ed., Resume des observations reunies, au Kwango, au sujet de deux affections d'origine indeterminee, Fonds reine Elisabeth, Brussels, pp. 1-36. |
|
|
World Health Organisation (WHO) (1996). Konzo: a distinct type of upper motor neuron disease. Weekly Epidemiol. Rec. 71:225-232 |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


