ABSTRACT
In this study, the infection of young children with Mycobacterium tuberculosis and drug-resistant M. tuberculosis in a mass gathering area in Al-Madinah Al-Munawwarah, was investigated and discussed. All the children, 15 years old and younger, who were referred to the central tuberculosis laboratory in Al-Madinah between January 2012 and December 2014 were included in this study. Among a total of 622 registered new cases, 68 (10.9%) were children, males were 40 (58.8%) while 28 (41.2 %) were females. All the children were vaccinated with Bacillus Calmette-Guérin (BCG) within their first week of birth. Sixty (88.2%) children were infected with M. tuberculosis, whereas 8 (11.8%) had non tuberculous mycobacteria (NTM). Clinically, pulmonary tuberculosis was confirmed in 20 (29.4%) cases, whereas the remaining 48 (70.6%) had extra pulmonary tuberculosis. Multidrug-resistant M. tuberculosis (MDR) was isolated from 3 (4.4%) cases, all of whom were younger than five years; one with pulmonary and two with extrapulmonary tuberculosis. All the isolated MDR organisms belonged to the M. tuberculosis complex. The rates of mono-resistance to isoniazid (H), streptomycin (S), ethambutol (E) and pyrazinamide (Z) were 5.9, 1.5, 5.9 and 8.8%, respectively. No case was registered as mono-resistant to rifampin (R). The prevalence of childhood tuberculosis in the current study area is higher than the globally estimated rate. Since all the cases were new, MDR-TB was mostly due to infection with originally MDR strains.
Key words: Mycobacteria, polymerase chain reaction, resistance, antibiotics, antimicrobials.
Tuberculosis represents the leading cause of death from a single infectious agent, ranking above HIV/AIDS. Moreover, it is the ninth leading cause of death worldwide. According to the WHO, 10.4 million cases of TB were present in 2016; an estimated 1.3 million deaths occurred amongst HIV-negative patients, and an additional 0.374 million deaths occurred amongst HIV-ositive patients (WHO, 2017). Most cases (90%) were adults, and 65%
were males. Regarding drug resistance, 0.6 million new cases with resistance to rifampicin (RRTB) were registered in 2016, of which 0.49 includedmultidrug-resistant TB (MDR-TB) (WHO, 2017).
The prevalence of tuberculosis amongst children is always underestimated (Starke, 2002) because of several factors, the most important of which is difficulty in diagnosis (Hailu et al., 2014). Children are not usually considered a significant source of disease transmission; thus, they are neglected by national control programmes (Marais and Pai, 2007).
Multidrug-resistant tuberculosis is defined as TB caused by Mycobacterium tuberculosis which is resistant to both rifampicin and isoniazid (WHO, 2008). According to the WHO, the rate of MDR-TB is increasing; because children represent 20% of TB-infected population in high-burden countries (Marais et al., 2006a). It is likely that the prevalence of MDR-TB amongst children is also increasing. The most probable source of infection amongst children is their household contacts; however, routine investigations during surveillance in areas with low resources and high burden of tuberculosis are rare (Hill and Ota, 2010; Hwang et al., 2011). The transmission of drug resistant bacilli from close contact is also a key explanation of MDR-TB in children (Shah and Chilkar, 2012).
The diagnosis of paediatric TB is difficult with regard to microbiological tools because this disease can only be detected in approximately 2 to 40% of all radiologically confirmed pulmonary TB cases (Zar et al., 2005), and it rarely increases above 50% unless extensive disease is present (Marais et al., 2006b); therefore, the treatment of children is usually based on symptoms and radiology, presuming drug-susceptibility (WHO, 2006). In general, physicians do not employ treatment options for MDR-TB without confirmation via microbiological tools because of the prolonged treatment duration and the adverse effect of drugs that might require hospitalisation.
Recent reports regarding the prevalence and incidence of TB in the Kingdom of Saudi Arabia (KSA) have shown variable rates in different regions of the country (8.5 to 23.1%) amongst Saudi nationals; however, the percent has increased in the Makkah region (38%) amongst non-Saudis (Abouzeid et al., 2012; Gleason et al., 2012). Improvements in healthcare have reduced the incidence of TB; however, its prevalence remains high primarily because of the large populations generated by the Hajj and Omarah events (Shibl et al., 2013).
Regarding MDR in KSA, the 2013 WHO estimates revealed previously treated and new case rates of 5.5 and 0.51%, respectively. Several studies conducted throughout KSA showed 14-20% resistance rates to first-line drugs and 1-44% resistance rates to MDR-TB (Al-Rubaish et al., 2001; Abu-Amero, 2002; Al-Hajoj et al., 2007). This study aimed to investigate the prevalence of tuberculosis and MDR Mycobacterium tuberculosis among children in Al-Madinah Al-Monawwarah, KSA.
Study type, population and sampling
This study included all newly confirmed tuberculosis patients of age 15 years and below (n = 68/622; 10.9%), who were referred to the central tuberculosis laboratory in Al-Madinah Al-Munawwarah between January 2012 and December 2014. Informed consent documents were offered to their parents. Basic demographic data were collected.
Sputum specimens were collected from some of the pulmonary tuberculosis enrolled patients and processed using standard procedures. In patients with extrapulmonary tuberculosis, fine needle aspirates were collected; in other cases, gastric lavage samples were collected from infants.
Isolation and identification of mycobacterium
Ziehl-Neelsen stain (ZN)
ZN staining was performed on all collected specimens using standard measures. Following absolute alcohol fixation, carbolfuchsin was poured over a smear and heated gently until boiling for 5 min and then washed off with water. Then, 20% sulphuric acid was added, left for one min and washed off with water. Methylene blue was added for two min, and the sample was again washed with water. Finally, the slides were allowed to air dry, and they were examined under an oil immersion lens (Olympus, Japan) for acid fast bacilli.
Drug-susceptibility testing via BACTEC MGIT 960
Specimens from the 68 patients were cultured in a Mycobacteria Growth Indicator Tube (MGIT) 960 system (Becton Dickinson Microbiology System, USA). The cultures were further investigated for susceptibility to anti-tuberculosis drugs as directed by the manufacturer using an M960 system. The final drug concentrations used for drug susceptibility testing (DST) were E, 5.0 mg/ml; S, 0.1 mg/ml; R, 1.0 mg/ml; H, 0.1 mg/ml; and Z, 25 mg/ml. For each isolate, a growth tube (a growth supplement without a drug) was included as a control to determine the relative growth ratio, and the M960 system was used to report the results of the DST.
GenXpert MTB/RIF assay
An MTB/RIF assay was conducted according to Blakemore et al. (2010) by using GeneXpert (Cepheid, Sunnyvale, CA). Briefly, three volumes of sample reagent were added to one volume of sample, and the container was shaken and kept at room temperature for 15 min. Then, 2 ml of the mixture was transferred to the test cartridge. Samples with suspicious results (those that differed in culture from those in GenXpert or vice versa) were re-checked.
GenXpert negative samples were subjected to further identification using conventional methods including ZN staining, and the follow-up cultures were created on Lowenstein Jensen (LJ) medium to identify NTM (Gangadharam, 1996).
Data analysis
The Statistical Package for Social Sciences (SPSS), version 21.0 (SPSS Inc., Chicago, IL, USA, 2012), was used for all data analyses. A two-tailed P-value of < 0.05 was considered as significant.
Epidemiological findings and risk factors
Between January 2012 and December 2014, 68 children (<15 years old) of 622 cases (10.9%) referred to the tuberculosis reference laboratory in Al-Madinah Al-Munawwarah were enrolled in this study. All cases were confirmed and registered as new, and all received a postnatal BCG vaccination. Regarding nationality, 64 (94.1%) of the patients were Saudis, whereas only 4 (5.9%) were foreign nationals.
This study included 40 males and 28 females, with a male/female ratio of 1.4:1. Despite the lower number of females as compared to males, this difference was not significant. The sample was divided into 3 age groups: 25 (36.8%) infants ≤ 1 year old, 17 (25%) 2- to 5-year-old and 26 (38.2 %) 6- to 15-year-old patients.
Diagnosis was conducted via ZN smear, culture and PCR. Table 1 shows the demographic data of the patients and the smear results, whereas Figure 1 shows the results of the different methods used for diagnosis.
Isolation and identification of M. tuberculosis
Positive ZN smears were recorded in 24 (35.3%) cases, with a sensitivity that was significantly lower than the culture (P < 0.001). All the cultures tested positive, and 8 of the cultured isolates (11.8%) were rapid growers and tested negative in PCR (GenXpert). The cultures were identified with the aid of biochemical reactions as nontuberculous mycobacteria (NTM) (Table 2) and the remaining 60 (88.2%) were labelled M. tuberculosis.
Extrapulmonary tuberculosis
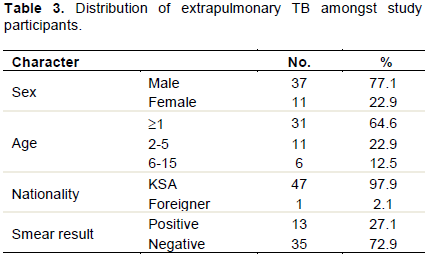
Extrapulmonary tuberculosis (EPTB) was significantly more prevalent than pulmonary tuberculosis (P < 0.001), which was found in 48 (70.6%) of the cases, whereas only 29.4% had PTB. The distribution of extrapulmonary cases in the sample is shown in Table 3. Samples for extrapulmonary TB included fine needle lymph node aspirates, pus and gastric lavage. Nearly two third of the extrapulmonary cases (31/48; 64.6%) were infants of age range of 1 month - 1 year. In addition, two of the extrapulmonary TB cases (4.2%) were due to NTM (Table 2).
Drug-susceptibility testing
The mono-drug resistance to antibacterial agents considered as the first-line treatment for tuberculosis was determined. Of the 68 isolates, 6 (8.8%) were resistant to pyrazinamide, 4 (5.9%) were resistant to isoniazid, 4 (5.9%) were resistant to ethambutol, and 1 (1.5%) was resistant to streptomycin; however, no mono-resistance was noted against Rifampin. Poly-drug resistance was found in 5 (7.4%) of the isolates, and MDR was found in 3 (4.4%) of the isolates. Table 4 shows the resistance patterns to isoniazid, pyrazinamide, ethambutol, rifampin and streptomycin.
In this study, MDR was diagnosed in 3/68 (4.4%) patients; one was isolated from a five-month-old Saudi male with pulmonary tuberculosis, and the other two were isolated from 2- and 4-year-old Saudi males with extrapulmonary TB. Table 5 presents the distribution of MDR among the study population while Table 6 shows the microbiological and demographic data of these MDR cases.
Tuberculosis remains the infectious disease with the highest morbidity rate (WHO, 2017). It is not well recorded amongst children (Starke, 2002) because of the difficulty associated with its diagnosis (Hailu et al., 2014). Children are usually expected to contract the infection from their household contacts (Hwang et al., 2011, Hill et al., 2010).
In this study, 622 patients referred to the central tuberculosis laboratory in Al-Madina were included after giving their informed consent. Among them, 68 (10.9%) children of the age of 15 years and less were present. The percent of paediatric TB found in the current study is higher than the expectations of the WHO, which recorded a 6% infection rate amongst children (WHO, 2014). However, it is well documented that only 50% of paediatric TB cases are recorded (Joshi et al., 2015); moreover, the actual percentage of infected children is approximately 11% (Nelson and Wells, 2004). In this context, this stiudy finding is within the normal range. However, active case finding is recommended through several means including screening of household contacts, providing better motherhood healthcare services and the screening of schoolchildren (Joshi et al., 2015).
In this study, NTM were found in 11.8% of the studied children population. This result differs from those obtained in Italy, where 62.9% of the mycobacterial infections of the head and neck in children were due to NTM (Caruso et al., 2009). This discrepancy might be because of several social, environmental or genetic factors.
The age groups did not significantly differ with regard to susceptibility to the infection. However, children less than one year old comprised 36.8% of the sample, which is more than one-third of the total. Given that the age range of the remaining patients is 2-15 years, this frequency is relatively high. Differences in the immune response that account for the difference in the national history of the disease might explain this high frequency of children less than one year of age (Piccini et al., 2014; Starke, 2004). Before two years of age, the primary infection leads to the rapid onset of the disease with severe symptoms, whereas disease progression is less likely in young children (Marais et al., 2004).
In this study, ZN smears were positive only in 35.3% of the study subjects. Because of the difficulty in collecting specimens from children (fine needle use, gastric aspiration and sputum collection, which is not spontaneously induced in children), it is agreed internationally that TB diagnosis is an obscure area of research that generally involves inaccurate and slow diagnoses (Graham et al., 2014; Marais et al., 2013).
In this study, 70.6% of the cases were identified as extrapulmonary tuberculosis while only 29.4% had PTB. Nearly two-thirds of the extrapulmonary cases (31/48; 64.6%) were infants with an age range of 1 month to 1 year. In addition, two of the extrapulmonary TB cases (4.2%) were due to NTM. This result does not match those of previous studies from other parts of the world including the USA, Turkey, Denmark, Italy and South Africa, where PTB was more prevalent than EPTB (Marais et al., 2006c; Peto et al., 2009; Buonsenso et al., 2012; Pekcan et al., 2013; Hatleberg et al., 2014). Because more than two-thirds of the patients in this study had EPTB, this finding alone suggests the possibility of under diagnosing EPTB in the absence of pulmonary evidence of the disease. It is well agreed worldwide that TB remains a major challenge because EPTB has a silent onset and difficult microbiological confirmation measures (Devrim et al., 2014). However, the bright side of EPTB in this study is that most of the cases presented with the least deleterious clinical form, lymphadenopathy. This result corroborates those of other studies (Devrim et al., 2014; Buonsenso et al., 2012). Moreover, none of the cases were recorded as TB meningitis in this study. The low incidence of CNS TB is mostly attributable to the high BCG vaccination rate (Devrim et al., 2014; Abubakar et al., 2013); in fact, almost all of the participants were vaccinated. Another factor that might influence EPTB is age because children less than 5 years old have a greater tendency to develop EPTB than older children (Cruz and Starke, 2010). In this study, 64.6% of children with EPTB were less than 1 year old, and 22.9% were between 2 and 5 years old, for an overall rate of 87.5%. This result corroborates those of other reports (Cruz and Starke, 2010).
The resistance to isoniazid was 5.9%, whereas the total resistance (either to isoniazid alone or combined with another drug) was 17.6%, making this important anti-tuberculosis therapy a target for the highest resistance rate. Isoniazid resistance in children is a worldwide phenomenon with variability in its frequency depending on geographical region (Devrim et al., 2014; Yuen et al., 2013; Dilber et al., 2000). In 2015, the global estimate of isonizid resistance amongst children was 12.1%, with higher rates in the west Pacific, southeast Asia and Europe, with the latter harbouring a rate that exceeds 26.1% (Yuen et al., 2015); thus, the current finding is within the regional and global levels.
The resistance to pyrazinamide in the current study was 11.7%. A retrospective cohort study from the USA revealed a resistance rate of 1.8% amongst the isolates tested with regard to this antimicrobial agent. This rate is much lower than that of the present study; in the American study, however, the target population included all age groups (not only children); although, the authors concluded that an association exists between mono-resistance to pyrazinamide and extrapulmonary TB, they did not find a relationship between resistance to pyrazinamide and mortality or MDR burden (Budzik et al., 2014). The current study partially corroborates these results because no association between resistance to pyrazinamide and MDR was found.
In this study, MDR was diagnosed in 3/68 (4.4%). This percentage is similar to the international value reported by the WHO in 2014 (3.5%) amongst new cases (WHO, 2014). It is also similar to the results of a recent study conducted in the same area (Elhassan et al., 2017) and other areas throughout KSA (Varghese et al., 2013), although these studies included participants of all age groups. However, this value is lower than the MDR rate amongst children in other parts of the world such as Mexico, where 11.1% of children are diagnosed as having MDR-TB. The authors of that study attributed this finding to several possible factors, the most important of which is drug failure (Parra et al., 2011) which is not applicable in the current study.
Drug resistance can be attributed to several factors including genetic mutations, inadequate treatment, past treatment (Shah and Rahangdale, 2011) or the transmission of drug-resistant strains from close contact (Shah and Chilkar, 2012). Since all the participants were new cases in this study, approximately two-thirds were less than 5 years old, and 94% were Saudi nationals (that is, non-immigrants from countries with high TB burdens), the most likely source of infection is close contact. Hence, case finding and household contact screening might provide an effective control measure for limiting paediatric TB and paediatric MDR-TB in this area.
The authors have not declared any conflict of interests.
REFERENCES
|
Abouzeid MS, Zumla, A, Felemban S, Alotaibi B, O'Grady J, Memish ZA (2012). Tuberculosis trends in Saudis and non-Saudis in the kingdom of Saudi Arabia-a 10 year retrospective study (2000-2009). PLoS One 7:e39478.
Crossref
|
|
|
|
Abu-Amero KK. (2002). Status of antituberculosis drug resistance in Saudi Arabia 1979-98. East Mediterr Health Journal 8:664-670.
|
|
|
|
|
Abubakar I, Pimpin L, Ariti C, Beynon R, Mangtani P, Sterne JA, Fine PE, Smith PG, Lipman M, Elliman, D., Watson JM, Drumright N, Whiting PF, Vynnycky E, Rodrigues LC (2013). Systematic review and meta-analysis of the current evidence on the duration of protection by bacillus Calmette-Guerin vaccination against tuberculosis. Health Technology Assessment 17:1-372.
Crossref
|
|
|
|
|
Al-Hajoj SA, Zozio T, Al-Rabiah F, Mohammad V, Al-Nasser M, Sola C Rastogi N (2007). First insight into the population structure of Mycobacterium tuberculosis in Saudi Arabia. Journal of Clinical Microbiology 45:2467-2473.
Crossref
|
|
|
|
|
Al-Rubaish AM., Madania AA, Al-Muhanna FA (2001). Drug resistance pulmonary tuberculosis in the Eastern Province of Saudi Arabia Saudi Medical Journal 22:776-779.
|
|
|
|
|
Blakemore R, Story E, Helb D, Kop J, Banada P, Owens M, Chakravort S, Jones M, Alland D (2010). Evaluation of the analytical performance of the Xpert MTB/RIF assay. Journal of Clinical Microbiology 48:2495-2501.
Crossref
|
|
|
|
|
Budzik JM, Jarlsberg LG, Higashi J, Grinsdale J, Hopewell P, Kato-Maeda M, Nahid P (2014). Pyrazinamide resistance, Mycobacterium tuberculosis lineage and treatment outcomes in San Francisco, California. PLoS One 9:95645.
Crossref
|
|
|
|
|
Buonsenso D, Lancella L, Delogu G, Krzysztofiak, A., Testa A, Ranno O, D'Alfonso P. Valentini P (2012). A twenty-year retrospective study of pediatric tuberculosis in two tertiary hospitals in Rome. Pediatrics Infectious Diseases 31:1022-1026.
|
|
|
|
|
Caruso G, Passali FM, Salerni L, Molinaro G, Messina M (2009). Head and neck mycobacterial infections in pediatric patients. International Journal of Pediatric Otorhinolaryngology 73:38-S41.
Crossref
|
|
|
|
|
Cruz AT. Starke JR (2010). Pediatric tuberculosis. Pediatrics Review 31:13-25.
Crossref
|
|
|
|
|
Devrim I, Akturk H, Bayram N, Apa H, Tulumoglu S, Devrim F, Erdem T, Gulfidan G, Ayhan Y, Tamsel I, Can D, Alper H (2014). Differences between pediatric extra-pulmonary and pulmonary tuberculosis: a warning sign for the future. Mediterranean Journal of Hematology and Infectious Diseases 6:2014058.
Crossref
|
|
|
|
|
Dilber E, Göçmen A, Kiper N, Ozçelik U (2000). Drug-resistant tuberculosis in Turkish children. Turkish Journal of Pediatrics 42:145-147.
|
|
|
|
|
Elhassan MM, Hemeg HA, Elmekki MA, Turkistani KA Abdul-Aziz AA (2017). Burden of multidrug resistant Mycobacterium tuberculosis among new cases in Al-Madinah Al-Monawarah, Saudi Arabia. Infectious Disorders - Drug Targets 17:14-23.
Crossref
|
|
|
|
|
Gangadharam PR (1996). Microbiology of nontuberculosis mycobacteria. Seminars in Respiratory Infections 11:231-243.
|
|
|
|
|
Gleason JA, McNabb SJN, Abduljadayel N, Abouzeid MS, Memish ZA (2012). Tuberculosis trends in the kingdom of Saudi Arabia, 2005 to 2009. Annals of Epidemiology 22:264-269.
Crossref
|
|
|
|
|
Graham SM (2014). Chest radiography for diagnosis of tuberculosis in children: a problem of interpretation. International Journal of Tuberculosis and Lung Disease 18:757.
Crossref
|
|
|
|
|
Hailu D, Abegaz WE, Belay M (2014). Childhood tuberculosis and its treatment outcomes in Addis Ababa: a 5-years retrospective study. BMC Pediatrics 14(1):61.
Crossref
|
|
|
|
|
Hatleberg CI, Prahl JB, Rasmussen JN, Andersen PH, Bjerrum S, Thomsen VO, Johansen IS (2014). A review of paediatric tuberculosis in Denmark: 10-year trend, 2000-2009. European Respiratory Journal 43:863-871.
Crossref
|
|
|
|
|
Hill PC, Ota MO (2010) Tuberculosis case-contact research in endemic tropical settings: design, conduct, and relevance to other infectious diseases. Lancet Infectious Diseases 10:723-732.
Crossref
|
|
|
|
|
Hwang TJ, Ottmani S, Uplekar M (2011). A rapid assessment of prevailing policies on tuberculosis contact investigation. International Journal of Tuberculosis and Lung Disease 15:1620-1623.
Crossref
|
|
|
|
|
Joshi B, Chinnakali P, Shrestha A, Das M, Kumar A, Pant R, Lama R, Sarraf R, Dumre S, Harries A (2015). Impact of intensified case-finding strategies on childhood TB case registration in Nepal. Public Health Action 5:93-98.
Crossref
|
|
|
|
|
Marais BJ, Gie RP, Schaaf HS, Hesseling AC, Obihara CC, Starke,JJ, Enarson DA, Donald PR, Beyers N (2004). The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. International Journal of Tuberculosis and Lung Disease 8:392-402.
|
|
|
|
|
Marais BJ, Hesseling AC, Gie RP, Schaaf HS, Beyers N (2006a). The burden of childhood tuberculosis and the accuracy of community-based surveillance data. International Journal of Tuberculosis and Lung Disease 10:259-263.
|
|
|
|
|
Marais BJ, Hesseling AC, Gie RP, Schaaf HS, Enarson DA, Beyers N (2006b). The bacteriologic yield in children with intrathoracic tuberculosis. Clinical Infectious Diseases 42:69-e71.
Crossref
|
|
|
|
|
Marais BJ, Gie RP, Schaaf HS, Hesseling AC, Enarson DA, Beyers, N (2006c) The spectrum of disease in children treated for tuberculosis in a highly endemic area. International Journal of Tuberculosis and Lung Disease 10:732-738.
|
|
|
|
|
Marais BJ, Pai M (2007). Recent advances in the diagnosis of childhood tuberculosis. Archives of Disease in Childhood 92:446-452.
Crossref
|
|
|
|
|
Marais BJ, Graham SM, Maeurer M, Zumla A (2013) Progress and challenges in childhood tuberculosis. Lancet Infectious Diseases 13:287-289.
Crossref
|
|
|
|
|
Nelson J, Wells CD (2004). Global epidemiology of childhood tuberculosis. International Journal of Tuberculosis and Lung Disease 8:636-647.
|
|
|
|
|
Parra MM, Rodriguez JK, Garcia JLA, Lopez-Vidal Y, Castanon-Arreola M, Balandrano S, Rastogi N, Castrellon PG (2011). Mycobacterium tuberculosis complex genotype diversity and drug resistance profiles in a pediatric population in Mexico. Tuberculosis Research and Treatment P 239042.
|
|
|
|
|
Pekcan S, Aslan AT, Kiper N, Uysal G, Gurkan F, Patiroglu T, Ozturk M, Ozen M, Dagli E, Dogru U, Kocabas E, Sarisoy O, Kocak A, Uzuner N, Reisli I, Bolat A, Uguz A, Karakelleoglu C, Uyan A, Kose M, Cinel G, Cobanoglu N, Yalcin E, Dogru D, Ozcelik U (2013). Multicentric analysis of childhood tuberculosis in Turkey. Turkish Journal of Pediatrics 55:121-129.
|
|
|
|
|
Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR (2009). Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clinical Infectious Diseases 49:1350-1357.
Crossref
|
|
|
|
|
Piccini P, Chiappin E, Tortoli, E, de Martino M, Galli L (2014). Clinical peculiarities of tuberculosis. BMC Infectious Diseases 14:S4.
Crossref
|
|
|
|
|
Shah I, Chilkar S (2012). Clinical profile of drug resistant tuberculosis in children. Indian Pediatrics 49:741-744.
Crossref
|
|
|
|
|
Shah I, Rahangdale A (2011). Partial extensively drug resistance (XDR) tuberculosis in children. Indian Pediatrics 48:977-979.
|
|
|
|
|
Shibl A, Tufenkeji H, Khalil M, Memish Z (2013). Consensus recommendation for meningococcal disease prevention for Hajj and Umra pilgrimage/travel medicine. Eastern Mediterranean Health Journal 19:389-392.
Crossref
|
|
|
|
|
Starke JR (2002). Childhood tuberculosis: ending the neglect. International Journal of Tuberculosis and Lung Disease 6:373-374.
|
|
|
|
|
Starke JR (2004). Tuberculosis in children. In Seminars in Respiratory and Critical Care Medicine. New York, NY: Thieme Medical Publishers, Inc.
Crossref
|
|
|
|
|
Varghese B, Supply P, Allix-Beguec C, Shoukri M, Al-Omari R, Herbawi M, Al-Hajoj S (2013). Admixed phylogenetic distribution of drug resistant Mycobacterium tuberculosis in Saudi Arabia. PLoS One 8:e55598.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2006). Guidance for National Tuberculosis Programmes on the Management of Tuberculosis in Children. WHO/ HTM/TB/2006371, WHO/FCH/CAH/20067. Geneva, Switzerland: WHO.
|
|
|
|
|
World Health Organization (WHO) (2008). Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis—Emergency Update. WHO/HTM/TB/2008402. Geneva, Switzerland: WHO.
|
|
|
|
|
World Health Organization (WHO) (2014). Global Tuberculosis Report 2014. Geneva: WHO.
|
|
|
|
|
World Health Organization (WHO) (2017). Global tuberculosis report 2017.Geneva: WHO.
|
|
|
|
|
Yuen CM, Jenkins, HE, Rodriguez CA, Keshavjee S, Becerra MC (2015). Global and regional burden of isoniazid-resistant tuberculosis. Pediatrics 136:50-e59.
Crossref
|
|
|
|
|
Yuen CM, Tolman AW, Cohen T, Parr JB, Keshavjee S, Becerra MC (2013). Isoniazid-resistant tuberculosis in children: a systematic review. Review. Pediatric Infectious Disease Journal 32:217-e226.
Crossref
|
|
|
|
|
Zar HJ, Hanslo D, Apolles P, Swingler G, Hussey G (2005). Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. Lancet 365:130-134.
Crossref
|
|