Full Length Research Paper

ABSTRACT
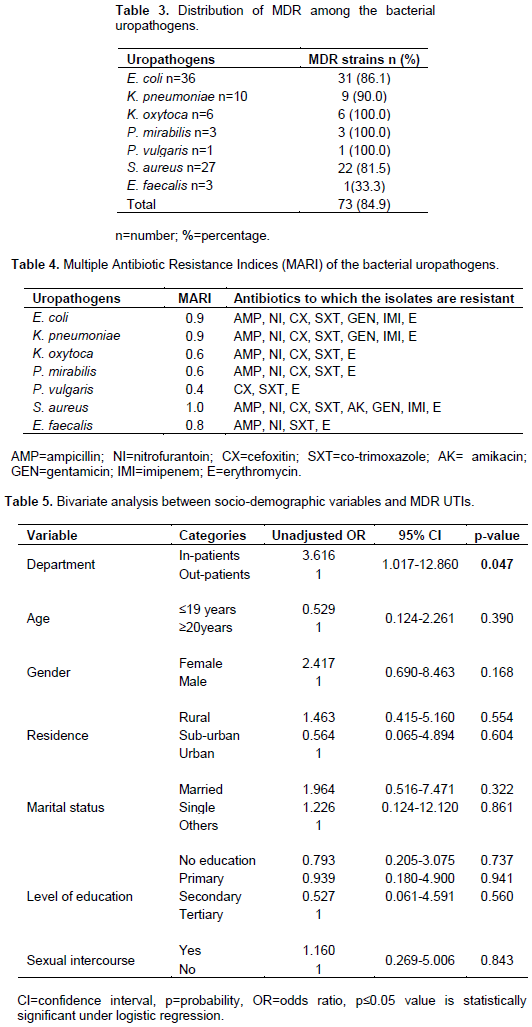
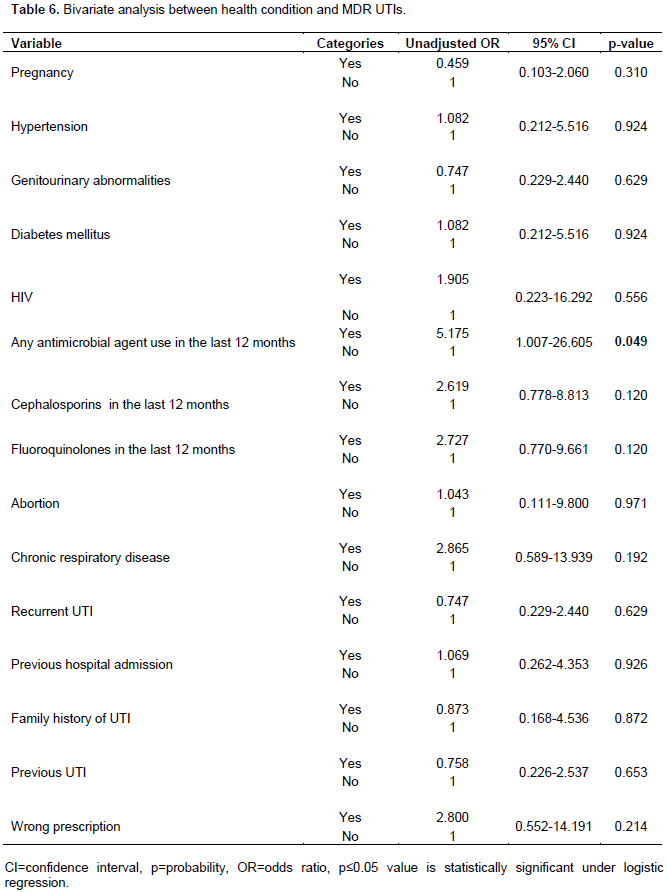
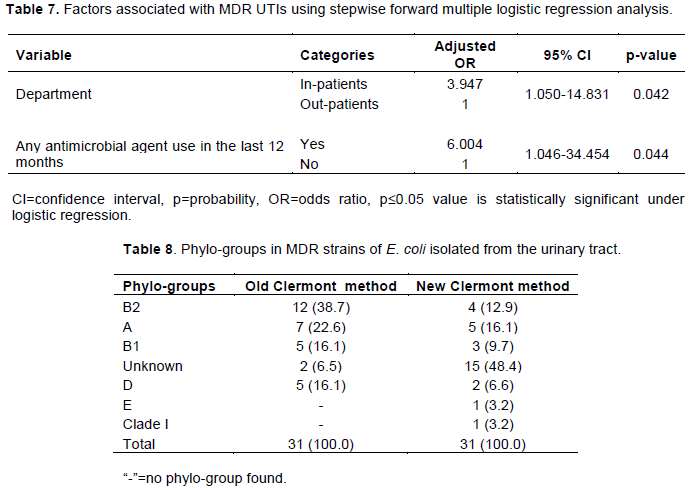
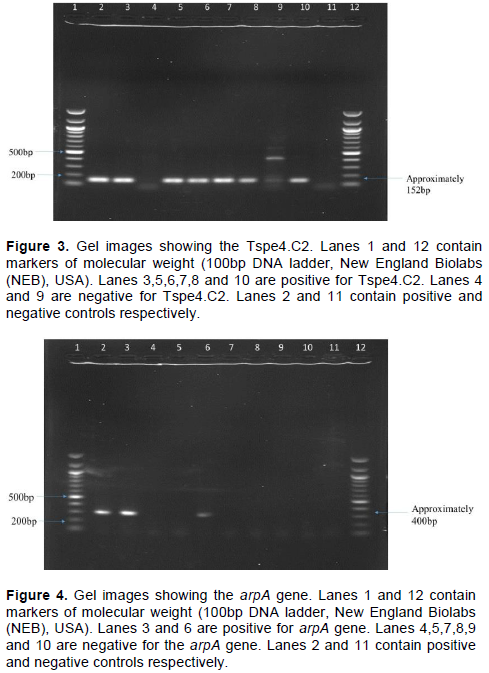
Due to the increasing rates of multidrug resistance (MDR) among the Enterobacteriaceae that cause urinary tract infections (UTIs), selection of antimicrobial agents for empirical therapy is becoming a major challenge. This study determines the antimicrobial resistance profiles, multidrug resistance profiles, multiple antibiotic resistance indices (MARI), factors associated with MDR UTIs and the phylogenetic groups of MDR Escherichia coli strains isolated from the urinary tract among patients attending hospitals in Bushenyi District, Uganda. In this cross-sectional study, a total of 86 bacterial uropathogens isolated from 267 study participants suspected to have UTIs were subjected to antimicrobial susceptibility tests using the Kirby Bauer Disk diffusion method. Data for the factors associated with MDR was obtained by the use of questionnaires. Phylogenetic groups of the MDR E. coli were determined using the new Clermont method for phylotyping E. coli. Descriptive and multiple logistic regression statistical tools were used to determine phylogenetic groups, and assess for statistically significant relationship between MDR UTIs and factors suspected to be associated with MDR UTIs respectively. The isolates assigned as group B2 9/12 (75.0%), B1 2/5 (40.0%) and A 2/7 (28.6%) by using the old Clermont method could not be phylotyped using the new Clermont method and were grouped as non-typeable strains of E. coli. Our study demonstrates high prevalence of the non-typeable strains of MDR E. coli, we therefore recommend the use of modern DNA sequencing-based approaches which is the gold standard for genotyping bacteria, that this current study could not afford.
Key words: Phylogenetic analysis, bacterial urinary tract infections, factors associated with, multidrug resistance, Bushenyi District, Uganda.
INTRODUCTION
MATERIALS AND METHODS

RESULTS


DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
REFERENCES
|
Acaku M, Bwanga F, Boum Y, Bazira J (2014). Prevalence and Genotypic Characterization of Extended-Spectrum Beta-Lactamases Produced by Gram Negative Bacilli at a Tertiary Care Hospital in Rural South Western Uganda. British Microbiology Research Journal 4(12):1541. |
|
|
Adwan K, Jarrar N, Abu-Hijleh A, Adwan G, Awwad E (2014). Molecular characterization of Escherichia coli isolates from patients with urinary tract infections in Palestine. Journal of Medical Microbiology 63(2):229-234. |
|
|
Ali I, Shabbir M, Iman NU (2017). Antibiotics susceptibility patterns of uropathogenic E. coli with special reference to fluoroquinolones in different age and gender groups. Journal of Pakistan Medical Association 67:1161. |
|
|
Ampaire L, Butoto A, Orikiriza P, Muhwezi O (2015). Bacterial and Drug Susceptibility Profiles of Urinary Tract Infection in Diabetes Mellitus Patients at Mbarara Regional Referral Hospital, Uganda. Microbiology Research Journal International 9(4):1-5. |
|
|
Basu S, Mukherjee SK, Hazra A, Mukherjee M (2013). Molecular characterization of uropathogenic Escherichia coli: nalidixic acid and ciprofloxacin resistance, virulent factors and phylogenetic background. Journal of Clinical and Diagnostic Research 7(12):2727-2731. |
|
|
Cantón R, Morosini MI (2011). Emergence and spread of antibiotic resistance following exposure to antibiotics. FEMS Microbiology Reviews 35(5):977-991. |
|
|
Chika E, Ugwu M, Iroha I, Gugu T, Duru C, Eze P, Esimone C (2017). Detection and antimicrobial susceptibility of some gram negative bacteria producing carbapenemases and extended spectrum β-Lactamases. Journal of Immunology Research 2:064-069. |
|
|
Clermont O, Bonacorsi S, Bingen E (2000). Rapid and simple determination of the Escherichia coli phylogenetic group. Applied and Environmental Microbiology 66(10):4555-4558. |
|
|
Clermont O, Bonacorsi S, Bingen E (2004). Characterization of an anonymous molecular marker strongly linked to Escherichia coli strains causing neonatal meningitis. Journal of Clinical Microbiology 42(4):1770-1772. |
|
|
Clermont O, Christenson JK, Denamur E, Gordon DM (2013). The Clermont Escherichia coli phyloâ€typing method revisited: improvement of specificity and detection of new phyloâ€groups. Environmental Microbiology Reports 5(1):58-65. |
|
|
Clermont O, Lescat M, O'Brien CL, Gordon DM, Tenaillon O, Denamur E (2008). Evidence for a humanâ€specific Escherichia coli clone. Environmental Microbiology 10(4):1000-1006. |
|
|
CLSI (2018). Performance Standards for Antimicrobial Susceptibility Testing. 28th ed. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute. |
|
|
Dancer SJ (2014). Controlling hospital-acquired infection: focus on the role of the environment and new technologies for decontamination. Clinical Microbiology Reviews 27(4):665-690. |
|
|
D'Andrea MM, Literacka E, Zioga A, Giani T, Baraniak A, Fiett J, Sadowy E, Tassios PT, Rossolini GM, Gniadkowski M, Miriagou V (2011). Evolution and spread of a multidrug -resistant Proteus mirabilis clone with chromosomal AmpC - type cephalosporinases in Europe. Journal of Antimicrobial Agents and Chemotherapy 55(6):2735-2742. |
|
|
Ehinmidu JO (2003). Antibiotics susceptibility patterns of urine bacterial isolates in Zaria, Nigeria. Tropical Journal of Pharmaceutical Research 2(2):223-228. |
|
|
Ejrnaes K (2011). Bacterial characteristics of importance for recurrent urinary tract infections caused by Escherichia coli. Danish Medical Bulletin 58(4):B4187. |
|
|
Ekwealor PA, Ugwu MC, Ezeobi I, Amalukwe G, Ugwu BC, Okezie U, Stanley C, Esimone C (2016). Antimicrobial evaluation of bacterial isolates from urine specimen of patients with complaints of urinary tract infections in Awka, Nigeria. International Journal of Microbiology. |
|
|
Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, Moran GJ, Nicolle LE, Raz R, Schaeffer AJ, Soper DE (2011). International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clinical Infectious Diseases 52(5):e103-e120. |
|
|
Gupta K, Hooton TM, Stamm WE (2001). Increasing antimicrobial resistance and the management of uncomplicated community-acquired urinary tract infections. Annals of Internal Medicine 135(1):41-50. |
|
|
Hadifar S, Moghoofei M, Nematollahi S, Ramazanzadeh R, Sedighi M, Salehi-Abargouei A, Miri A (2016). Epidemiology of Multidrug Resistant Uropathogenic Escherichia coli in Iran: a Systematic Review and Meta-Analysis. Japanese Journal of Infectious diseases (JJID) 70:19-25. |
|
|
Hasan AS, Nair D, Kaur J, Baweja G, Deb M, Ag¬garwal P (2007). Resistance patterns of urinary isolates in a tertiary Indian hospital. Journal of Ayub Medical College Abbottabad 19(1):39-41. |
|
|
Iranpour D, Hassanpour M, Ansari H, Tajbakhsh S, Khamisipour G, Najafi A (2015). Phylogenetic groups of Escherichia coli strains from patients with urinary tract infection in Iran based on the new Clermont phylotyping method. BioMed Research International. |
|
|
Jehan M, Mahadev HRY, Akhtar S, Masood S (2015). The Frequency and Antibiotic Susceptibility Patterns of Uropathogens in a Low-Income Locality of Karachi. International Journal of Pathology 13(2):14-19. |
|
|
Kabugo D, Kizito S, Ashok DD, Kiwanuka AG, Nabimba R, Namunana S, Kabaka RM, Achan B, Najjuka FC (2016). Factors associated with community-acquired urinary tract infections among adults attending assessment centre, Mulago hospital Uganda. African Health Sciences 16(4):1131-1142. |
|
|
Kalluru S, Eggers S, Barker A, Shirley D, Sethi AK, Sengupta S, Yeptho K, Safdar N (2018). Risk factors for infection with multidrug-resistant organisms in Haryana, India. American Journal of Infection Control 46(3):341-345. |
|
|
Katongole SP, Christine O, Robert ADDMO, Philip G (2015). Prevalence and drug susceptibility of isolates of urinary tract infections among febrile under-fives in Nsambya Hospital, Uganda. Open Science Journal of Clinical Medicine 3(6):199-204. |
|
|
Khawcharoenporn T, Vasoo S, Singh K (2013). Urinary tract infections due to multidrug-resistant Enterobacteriaceae: prevalence and risk factors in a Chicago Emergency Department. Emergency Medicine International. |
|
|
Kibret M, Abera B (2011). Antimicrobial susceptibility patterns of E. coli from clinical sources in northeast Ethiopia. African Health Sciences 11(3):40-45. |
|
|
Kish L (1965). Survey sampling (No. 04; HN29, K5.). |
|
|
Kyabaggu D, Ejobi F, Olila D (2007). The sensitivities to first-line antibiotic therapy of the common urinary tract bacterial infections detected in urine samples at a hospital in metropolitan Kampala (Uganda). African Health Sciences 7(4). |
|
|
Laupland KB, Ross T, Pitout JDD, Church DL, Gregson, DB (2007). Community-onset urinary tract infections: a population-based assessment. Infection 35(3):150. |
|
|
Lescat M, Clermont O, Woerther PL, Glodt J, Dion S, Skurnik D, Djossou F, Dupont C, Perroz, G., Picard B, Catzeflis F (2012). Commensal Escherichia coli strains in Guiana reveal a high genetic diversity with host dependant population structure. Environmental Microbiology Reports 5(1):49-57. |
|
|
Li B, Webster TJ (2018). Bacteria antibiotic resistance: New challenges and opportunities for implantâ€associated orthopedic infections. Journal of Orthopaedic Research® 36(1):22-32. |
|
|
Mahato S, Mahato A, Yadav J (2018). Prevalence and identification of Uropathogens in eastern Nepal and Understanding their antibiogram due to multidrug resistance and ESBL. Asian Pacific Journal of Microbiology Research 2(1):9-17. |
|
|
Martin O, Adamu AA, JuliusT, Josephat NM, Eddie W, Charles DK, Ezera A, Joel Bazira B (2019). Prevalence of Bacterial Urinary Tract Infections and Associated Factors among Patients Attending Hospitals in Bushenyi District, Uganda. International Journal of Microbiology 8 p |
|
|
UNAS C, Mpairwe Y, Wamala S (2015). Antibiotic Resistance in Uganda: Situation Analysis and Recommendations. Uganda National Academy of Sciences, Kampala, Uganda P 107. |
|
|
MüÅŸtak HK, Günaydin E, Kaya Ä°B, Salar MÖ, Babacan O, Önat K, Ata Z, Diker KS (2015). Phylo-typing of clinical Escherichia coli isolates originating from bovine mastitis and canine pyometra and urinary tract infection by means of quadruplex PCR. Veterinary Quarterly 35(4):194-199. |
|
|
Mwaka AD, Mayanja-Kizza H, Kigonya E, Kaddu-Mulindwa D (2011). Bacteriuria among adult non-pregnant women attending Mulago hospital assessment centre in Uganda. African Health Sciences 11(2). |
|
|
Nseir S, Blazejewski C, Lubret R, Wallet F, Courcol R, Durocher A (2011). Risk of acquiring multidrug-resistant Gram-negative bacilli from prior room occupants in the intensive care unit. Clinical Microbiology and Infection 17(8):1201-1208. |
|
|
Odoki M, Aliero AA, Tibyangye J, Nyabayo MJ, Wampande E, Drago KC, Agwu E, Bazira J (2019). Prevalence of Bacterial Urinary Tract Infections and Associated Factors among Patients Attending Hospitals in Bushenyi District, Uganda. International Journal of Microbiology. |
|
|
Odoki M, Bazira J, Agwu E (2015). Health-point survey of bacteria urinary tract infections among suspected diabetic patients attending clinics in Bushenyi district of Uganda. Special Bacterial Pathogens Journal 1(1):1-5. |
|
|
Odongo CO, Anywar DA, Luryamamoi K, Odongo P (2013). Antibiograms from community-acquired uropathogens in Gulu, northern Uganda-a cross-sectional study. BMC (BioMed Central) Infectious Diseases 13(1):193. |
|
|
Oli AN, Iyinagolu RA, Ichoku UJ, Ugwu MC, Ezeobi I, Ejiofor OS, Anagu LO, Esimone CO (2013). Antibiotic susceptibility profile of community isolates of Staphylococcus aureus. Journal of Pharmaceutical Research and Opinion 3(7):42-47. |
|
|
Prakash D, Saxena RS (2013). Distribution and antimicrobial susceptibility pattern of bacterial pathogens causing urinary tract infection in urban community of Meerut city, India. ISRN Microbiology. |
|
|
Raymond B (2019). Five rules for resistance management in the antibiotic apocalypse, a road map for integrated microbial management. Evolutionary Applications 12(6):1079-1091. |
|
|
Regmi N, Kafle S, Paudyal R (2018). Multi-drug resistant uropathogens isolated from mid-stream urine samples. Journal of Institute of Science and Technology 23(1):39-42. |
|
|
Sáez-López E, Guiral E, Fernández-Orth D, Villanueva S, Goncé A, López M, Teixidó I, Pericot A, Figueras F, Palacio M, Cobo T (2016). Vaginal versus obstetric infection Escherichia coli isolates among pregnant women: antimicrobial resistance and genetic virulence profile. PLoS One 11(1). |
|
|
Sarowska J, Futoma-Koloch B, Jama-Kmiecik A, Frej-Madrzak M, Ksiazczyk M, Bugla-Ploskonska G, Choroszy-Krol I (2019). Virulence factors, prevalence and potential transmission of extraintestinal pathogenic Escherichia coli isolated from different sources: recent reports. Gut Pathogens 11(1):10. |
|
|
Shabbir M, Iman NU, Shah, M. Z (2018). Multidrug resistant uropathogens in urinary tract infections and their antibiotic susceptibility patterns. Journal of Medical Sciences 26(1):24-27. |
|
|
Stamm WE, Norrby SR (2001). Urinary tract infections: disease panorama and challenges. The Journal of Infectious Diseases 183(Supplement_1), S1-S4. |
|
|
Tambekar DH, Dhanorkar DV, Gulhane SR, Khandelwal VK, Dudhane MN (2006). Antibacterial susceptibility of some urinary tract pathogens to commonly used antibiotics. African Journal of Biotechnology 5(17). |
|
|
Tenney J, Hudson N, Alnifaidy H, Li JTC, Fung KH (2018). Risk factors for aquiring multidrug-resistant organisms in urinary tract infections: A systematic literature review. Saudi Pharmaceutical Journal 26(5):678-684. |
|
|
Tibyangye J, Okech MA, Nyabayo JM, Nakavuma JL (2015). In vitro antibacterial activity of Ocimum suave essential oils against uropathogens isolated from patients in selected hospitals in Bushenyi District, Uganda. British Microbiology Research Journal 8(3):489. |
|
|
Ugwu MC, Odimegwu DC, Ibezim EC, Esimone CO (2009). Antibiotic resistance patterns of Staphylococcus aureus isolated from nostrils of healthy human subjects in a southeastern Nigeria locality. Macedonian Journal of Medical Sciences 2(4):294-300. |
|
|
Ullah A, Syed RHS, Babiker SA, Shahida S (2018). Prevalence of symptomatic urinary tract infections and antimicrobial susceptibility patterns of isolated uropathogens in kohat region of Pakistan. Biology and Medicine 3(3):85-89.
UNAS C, Mpairwe Y, Wamala S (2015). Antibiotic Resistance in Uganda: Situation Analysis and Recommendations. Uganda National Academy of Sciences, Kampala, Uganda P 107. |
|
|
World Medical Association (WMA) Declaration of Helsinki (2000). Ethical Principles for Medical Research Involving Human Subjects, The 52nd WMA General Assembly, Edinburgh, Scotland. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


