Full Length Research Paper
ABSTRACT
Glaucoma is a major public health problem, being the leading cause of irreversible visual impairment worldwide. In most cases, glaucoma is associated with intraocular pressure (IOP) levels that are above those considered normal (IOP ≥ 21 mmHg). The aim of the present work is to describe the pattern of eye drops prescription in patients with glaucoma in the state of Sergipe, Brazil. A descriptive cross-sectional study with retrospective documentary analysis, developed at the Eye Institute of Sergipe was performed. Of all glaucoma patients, 41.5% had a family history of the disease. Among the popular drugs, Latanoprost 0.005% is the most requested totaling 34% of prescriptions. In the Region 2, a significant association (c2= 48, 45; p<0.05) was observed between monotherapy and high IOP. The present study showed that the pattern of eye drops prescription was as recommended by the Brazilian Society of Glaucoma. Although, these medications were distributed freely, most patients with glaucoma have high IOP. Therefore, considering the importance of glaucoma as the second cause of blindness worldwide it is essential to carry out studies that evaluate the factors that influenced the effectiveness of eye drops use for treatment of glaucoma.
Key words: Glaucoma, ophthalmic solutions, prescription drugs.
INTRODUCTION
Glaucoma is a silent chronic disease that is characterized by progressive alterations of the optic disc, retinal nerve fiber layer, irreversible loss of vision and damage to the optic nerve. In most cases, glaucoma is associated with intraocular pressure (IOP) levels that are above those that are considered normal (IOP ≥ 21 mmHg). The total number of patients (aged 40 - 80 years) with glaucoma worldwide was estimated to be 64.3 million in 2013 increasing to 111.8 million in 2040, especially in Asia, Africa and America (Tham et al., 2014). According to the World Health Organization (WHO), glaucoma accounts for 13% of global blindness, and 2.4 million new cases occur every year (WHO, 2004; WHO, 2013).
Although, glaucomatous damage is deemed irreversible, approximately 90% of the blindness caused by glaucoma could be avoided with early diagnosis and treatment (Susanna, 2015, UN, 2009). Thus, glaucoma is a serious public health problem (William et al., 2014). Depending on the condition, medical, laser, surgical treatments, and antiglaucoma therapy can be used.
A great number of topical medications are available for use in glaucoma treatment. These eye drops cause IOP reduction by either decreasing production of aqueous humor from the ciliary body, or increasing outflow of the aqueous humor through the trabecular meshwork or uveoscleral pathway, the natural drain of the eye (Sun et al., 2015).
In developing countries, including Asia, Africa and South America, most glaucoma patients are unconscious that they have the disease and visual injury that is also prevalent and severe (Thomas et al., 2012; Leite et al., 2011). Moreover, two reviews highlight that lack of adherence to the antiglaucoma therapy may culminate in the patient’s vision loss (Castro, 2009; Leite et al., 2011). The low adherence can be explained because the glaucoma medications do not improve vision, may have important side effects and are relatively expensive (Leite et al., 2011).
Data on the prevalence of the disease in Brazil are scarce (Leite et al., 2011; Castagno et al., 2009; Tham et al., 2014). Sakata et al. (2007) reported that the prevalence of glaucoma in South Brazilian population among people over 40 years old was 3.4%. According to Stillitano et al. (2005), the antiglaucoma therapy in Brazil is expensive, and only a fraction of the economically active population is treated. As reported by Brazilian Ministry of Health and Brazilian Council of Ophthalmology, about 2% of Brazilian population has glaucoma. Although since recently the Brazilian population has received free eye drops, more than one fifth of the glaucoma patients do not follow the drug treatment in an adequate technique (Castro, 2008, 2009). Then, this study aimed to characterize the use of eye drops in patients with glaucoma in part of Brazilian Northeast.
MATERIALS AND METHODS
Study design
The present study is a descriptive research that was based on secondary data extracted from medical records that were used by an ophthalmic reference center for glaucoma patients from the Brazilian Public Health Care System (SUS) in the State of Sergipe. The center attends to about 10,000 elderly patients, and its health care team consists of four physicians, one nurse, one nursing technician, and one pharmacist. Sergipe is the smallest state in Brazil, located in the Northeast Region, this is the second most populous and poorer region of the country.
Characterization of Brazilian health care
Since 1989, all 200,000 Brazilian have been entitled to free health care at primary, secondary, and tertiary level through a national health system that is unique in Latin America, being funded by taxes and social contributions, such as social security payments. The Brazilian Public Health Care System (SUS) has decentralized care coverage based on Family Health Strategy that proved to reduce common diseases, mortality, and reductions in unnecessary admissions (Victoria et al., 2011). This Health Care System is divided in territories called Health Regions.
The Health Regions represent the integration of actions and health services of the federative institutions in a territory to qualify the SUS management, and also to ensure integrity. It must be able to cover and solve almost all health needs shown by the population of the region. In this study, the Health Regions were divided into three regions. Each region has a specific number of municipalities: Region 1 (15), Region 2 (11) and Region 3 (10). The division of regions considers geographical proximity defined by cultural, economic and social aspects, provision of health services, communication networks and infrastructure (Duarte et al., 2015; Santos, 2015). In this context, the Brazilian Public Health Care System (SUS) has a Glaucoma Patient support program present in all States and municipalities in Brazil. This program aims to manage patient support, increase public access, and generate mechanisms that can expand the diagnosis, monitoring, and treatment of these patients (Brazil, 2002a,b).
Databases and analysis instrument
For monitoring glaucoma patients, databases including information on diagnosis and treatment were created. The databases included users who were diagnosed with primary open-angle glaucoma and who were treated between June 2011 and March 2012 in 36 municipalities. These municipalities covered 48%, nearly 1,000,000 inhabitants of the State of Sergipe. The analysis instrument was structured by researchers to evaluate the study population’s profile. The database analysis was performed by a team consisting of a pharmacist (C.A.S.S.) and a Pharmacy undergraduate student (C.B.R.) of the Federal University of Sergipe. Both researchers were trained for six hours in order to be able to evaluate the databases. The data collected included a sociodemographic profile for each patient (name, age, gender, and length of stay in the program), the drugs prescribed for ophthalmic use, comorbidity, prescription patterns and outcomes of the users that were monitored for ten months in an ophthalmic reference center. At the end of the study, all of the instruments used were reviewed by the two researchers (F.A.S. and D.P.L.J), the results were further analyzed.
Population of study
Data collection was obtained from medical records of 9,308 patients who were diagnosed with glaucoma. In order to characterize the prescription patterns of eye drops, the prescribed drugs and types of therapy were analyzed. In Brazil, the respondents reported their ethnicity for classification according to the Brazilian Institute of Geography (IBGE).
Statistics analysis
The data was analyzed with BioEstat 5.0 and Epi info for Windows, IOP (CDC, 2012) prevalence estimates were examined according to age and monotherapy (the use of a single drug to treat a particular disorder or disease). In order to evaluate the statistical significance of the association between these variables and IOP, Mantel-Haenszel chi-square test was employed. A confidence interval of 95% was set for all of the statistical tests performed, and the differences were considered statistically significant if the p value was equal to or lower than 0.05.
Ethical aspects
The study was approved by the research ethics commission of the federal university of sergipe with number CAAE: 06353912.1.0000.0058.
RESULTS
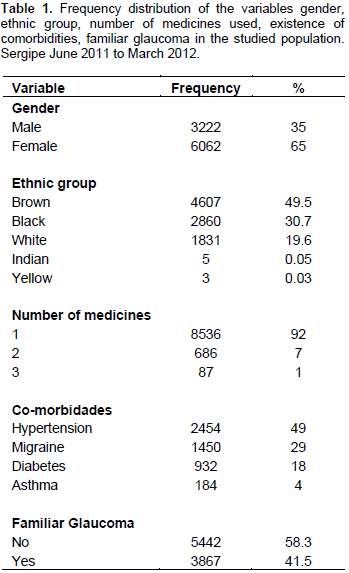
In this study, 65% of the patients were female. Most of the population reported themselves as brown-skinned (49%), 31% as black, and 20% were self-declared white as shown in Table 1. The average age of the population from the three regions was 58 years old (standard deviation: 15.81). Among the comorbidity more commonly reported by patients from the three regions, arterial hypertension, migraine, and diabetes had higher percentages of occurrence (49, 29, and 4%, respectively). In addition, 41.5% of the patients reported a family history of glaucoma as shown in Table 1.
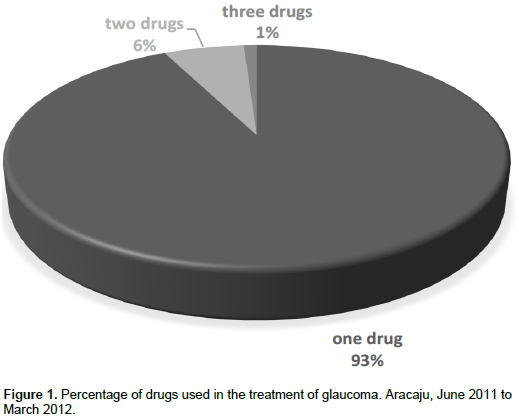
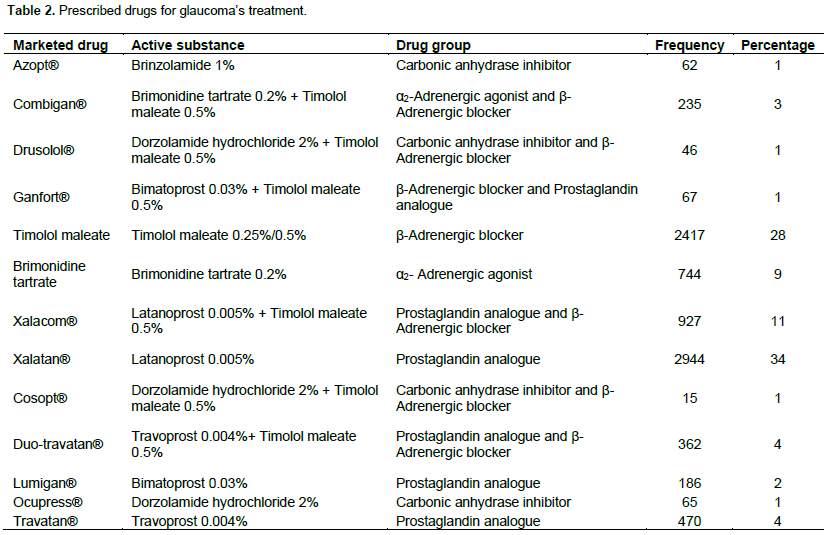
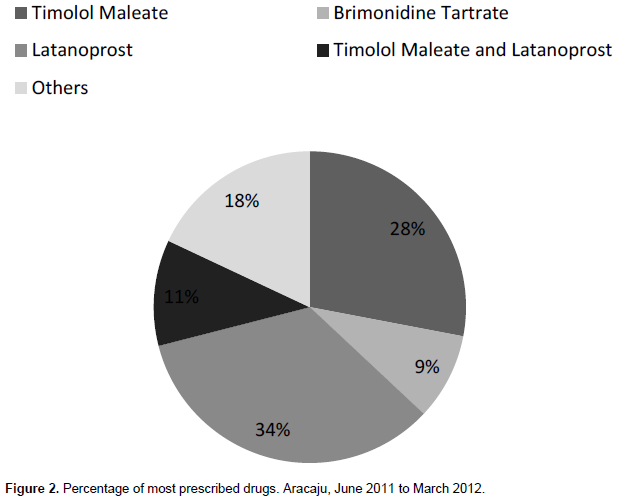
When comparing the average number of prescribed eye drops used by patients in the three regions, the majority (93% of the prescriptions) were for only one drug as shown in Figure 1. Thirteen drugs were used for the treatment of glaucoma as shown in Table 2, and prostaglandin analogs (Xalatan®) accounted 34% of the total as shown in Figure 2. In Region 2, a statistically significant association (c2 = 48.45; p < 0.05) was observed between monotherapy and abnormal IOP as shown in Table 3. Therefore, individuals with glaucoma who were treated with monotherapy were 1.76 times more likely to present an IOP ≥ 21 mmHg compared to individuals who were treated with more than one drug as shown in Table 3.

DISCUSSION
In this study, majority of the population was composed of female patients. Though, no associations between gender and the percentage of individuals affected by glaucoma have been reported, and the prevalence of the disease is similar in both genders (Lima et al., 2010). This phenomenon may be related to observations that women use healthcare services more often, especially for social and reproductive issues, which results in a greater demand of drugs by this gender (Quigley, 2006; Le A et al., 2003; Travassos et al., 2002; Fleith et al., 2008).
Regarding ethnicity, the majority of patients with glaucoma who were included in this study reported themselves as black or brown-skinned. According to the Brazilian glaucoma society (Brazil, 2009; Brazil, 2011; BCO, 2015), morbidity develops earlier in black-skinned individuals compared to whites. In this study, the majority of the patients were brown-skinned, and this could be related to the racial miscegenation in the state of Sergipe.
The most frequent comorbidity was arterial hypertension, but no correlation was found between glaucoma and systemic arterial hypertension. Although this study did not find any associations between these variables, several studies have reported a correlation of increased blood pressure and glaucoma susceptibility (Bonomi et al., 2000; Dielemans et al., 1995; Goldberg et al., 1981; Sun et al., 2012). The blue mountains eye study and rotterdam eye study reported an association between systemic arterial hypertension and glaucoma susceptibility (Mitchell et al., 2004; Hulsman et al., 2007). Although the percentage of patients with diabetes and glaucoma was small, the role of diabetes is important in glaucoma. Previous studies (Kanamori, 2004; Pasquale, 2006; Minwen, 2014) have suggested that people with diabetes are more likely to have high IOP and glaucoma. In a cross-sectional study, Bonovas et al. (2004) suggested that increased IOP is linearly correlated with the severity of diabetes.
This study showed that physicians initially prioritized treatment with only one drug, typically prostaglandin analogs, because prostaglandins and beta-blockers are recommended in the initial treatment of glaucoma (Heijl, 2002; Van der Valk et al., 2005; Li et al. 2006 Brazil, 2009; Burr et al., 2012; Estacia and Tognon, 2008). However, the analysis of the three regions showed that most of the patients in region 2 who were treated with only one drug had higher IOP values than the recommended standards. A reason for the lack of IOP control in this study may be a lack of adherence to the pharmacotherapy, as most of the patients reported eye irritation from the eye drops during the beginning of treatment in the medical records. In addition, several studies have reported that some patients who are diagnosed with glaucoma do not respond to first-line treatment drugs, and two or more antihypertensive drugs are required to achieve the target IOP (Cheng et al., 2012; Broadway and Cate, 2015; Kass, et al., 2002).
When analyzing the final IOP of the patients from Region 3, age was observed to be a risk factor for increased IOP. This conclusion was found to be in agreement with other studies that reported a positive association between high IOP and age (Kawai, 2001; Quigley, 2006; Schneck et al., 2004). Studies that were performed in Australia and the US have shown that the prevalence of the disease steadily increases with each decade of life, starting at 55 years old (Mitchell et al., 1996; Wensor, 1998; Quigley et al., 2001). Owsley (2011), in his research, describes the problems caused in vision due to aging and its impact on economic and personal life of the population.
The present study showed that, even though eye drops are prescribed for the treatment of glaucoma as recommended in the literature, patients have high IOP in the analyzed cities. These results could be associated to low adherence to glaucoma pharmacotherapy. Several studies have demonstrated that roughly 50% of patients were not adherent to their medication over 75% of the time (WHO, 2000; Okeke et al., 2009; Robin and Grover, 2011; Costa et al., 2011). Cohen et al. (2014) related that low adherence to glaucoma pharmacotherapy is related to patients, medication, physician and environmental factors. According to Robin and Grover (2011), some barriers influenced to adherence, such as forgetfulness, other priorities, lack of information and emotional factors. Another study carried out by Newman-Casey and colleagues (2015) also pointed to the difficulty with drop administration and the medication schedule as barriers associated with poor adherence, even in developing countries.
This study showed the prevalence among brown-skinned and elderly patients that use monotherapy of eye drop glaucoma. Although, these medications were distributed freely, most patients have high IOP. Because of the prevalence of glaucoma and the high costs of this disease, it is essential to perform further studies that adequately evaluate the factors that influenced the effectiveness of the use of eye drops, especially to patients’ knowledge and attitudes, in the treatment of glaucoma.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Bonomi L, Marchini G, Marraffa M, Bernardi P, Morbio R, Varotto A (2000). Vascular risk factors for primary open angle glaucoma: the Egna-Neumarkt Study. Ophthalmology 107(7):1287-93. |
|
|
Bonovas S, Peponis V, Filioussi K (2004). Diabetes mellitus as a risk factor for primary open-angle glaucoma: a meta-analysis. Diabetic medicine: J. Br. Diabetic Assoc. 21:609-614. |
|
|
Brazil (2002a). Assistance program for patients with glaucoma. Ministry of Health. Decree No. 867. |
|
|
Brazil (2002b). Assistance program for patients with glaucoma. Ministry of Health. Decree No. 338. |
|
|
Brazil (2011). Assistance program for patients with glaucoma. Ministry of Health. Decree No. 920. |
|
|
Brazilian Council of Ophthalmology BCO (2015). Information for the general public. 01:01-12. |
|
|
Brazilian Society of Glaucoma (2009). Brazilian Consensus Primary Angle Glaucoma Primary Open-Angle Glaucoma. 03:17-100. |
|
|
Broadway DC, Cate H (2015). Pharmacotherapy and Adherence Issues in Treating Elderly Patients with Glaucoma. Drugs Aging 32(7):569-581. |
|
|
Burr J, Azuara-Blanco A, Avenell A, Tuulonen A (2012). Medical versus surgical interventions for open angle glaucoma. Cochrane Database Syst. Rev. 9:Cd004399. |
|
|
Castagno VD, Fassa AG, Silva MCd, Carret MLV (2009). Shortage of ocular health care in the public system: a population-based study. Cad. Saúde Pública. 25(10):2260-2272. |
|
|
Castro ANBV, Mesquita WA (2008). Noncompliance with drug therapy of glaucoma (2008). Arq Bras Oftalmol. 71(2):207-214. |
|
|
Castro ANBV, Mesquita WA (2009). Noncompliance with drug therapy of glaucoma (2009): a review about intervening factors. Braz. J. Pharm. 45(3):453-459 |
|
|
CDC (2012). EPI Info™ for DOS vis. Atlanta: Centers for Disease Control and Prevention – Division of Public Health Surveillance and Informatics. |
|
|
Cheng JW, Cheng SW, Gao LD, Lu GC, Wei RL (2012). Intraocular pressure-lowering effects of commonly used fixed-combination drugs with timolol: a systematic review and meta-analysis. Plos One. 7:e45079. |
|
|
Cohen CO, Keinan BL, Geyer O, Milman U, Karkabi K (2014). Factors associated with adherence to glaucoma pharmacotherapy in the primary care setting. Fam Pract. 31(4):453-461. |
|
|
Costa KS, Barros MBA, Francisco PMSB, César CLG, Goldbaum M, Carandina L (2011). The use of medication and associated factors among adults living in Campinas, São Paulo, Brazil: differences between men and women. Cad. De Saúde Pública. 9(12):4909-4921. |
|
|
Dielemans I, Vingerling JR, Algra D, Hofman A, Grobbee DE, de Jong PT (1995). Primary open-angle glaucoma, intraocular pressure, and systemic blood pressure in the general elderly population. The Rotterdam Study. Ophthalmology 102:54-60. |
|
|
Duarte CMR, Pedroso MM, Belido JG, Moreira RS, Viacava F (2015). Regionalization and human development: a typology of health regions in Brazil. Cad. Saúde Pública. 31(6):1163-1174 |
|
|
Estacia P, Tognon T (2008). Considerations about administration angle of prostaglandin analogs. Arq. Bras. Oftalmol. 71(5):684-688. |
|
|
Fleith VD, Figueiredo MA, Figueiredo KFLRO, Moura EC (2008). Pattern of medicine consumption among users of the primary health care services in Lorena, SP. Ciênc. & Saúde Coletiva. 13:755-762. |
|
|
Goldberg I, Hollows FC, Kass MA, Becker B (1981). Systemic factors in patients with low-tension glaucoma. Br. J. Ophthalmol. 65(1):56-62. |
|
|
Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M (2002). Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 120(10):1268-1279. |
|
|
Hulsman CA, Vingerling JR, Hofman A, Witteman JC, de Jong PT (2007). Blood pressure, arterial stiffness, and open-angle glaucoma: the Rotterdam study. Arch Ophthalmol. 125(6):805-812. |
|
|
Kanamori A, Nakamura M, Mukuno H, Maeda H, Negi A (2004). Diabetes has an additive effect on neural apoptosis in rat retina with chronically elevated intraocular pressure. Curr. Eye Res. 28(1):47-54. |
|
|
Kass MA, Heuer DK, Higginbotham EJ, Johnson CA, Keltner JL, Miller JP, Parrish RK, Wilson MR, Gordon MO (2002). The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 120(6):701-713. |
|
|
Kawai SI, Vora S, Das S, Gachie E, Becker B, Neufeld AH (2001). Modeling of risk factors for the degeneration of retinal ganglion cells after ischemia/reperfusion in rats: effects of age, caloric restriction, diabetes, pigmentation, and glaucoma. FASEB J. 15(7):1285-1287. |
|
|
Le A, Mukesh BN, McCarty CA, Taylor HR (2003). Risk factors associated with the incidence of open-angle glaucoma: the visual impairment project. Invest Ophthalmol. Vis Sci. 44(9):3783-3789. |
|
|
Leite MT, Sakata LM, Medeiros FA (2011). Managing glaucoma in developing countries. Arq. Bras. Oftalmol. 74(2):83-84. |
|
|
Li N, Chen XM, Zhou Y, Wei ML, Yao X (2006). Travoprost compared with other prostaglandin analogues or timolol in patients with open-angle glaucoma or ocular hypertension: meta-analysis of randomized controlled trials. Clin. Exp. Ophthalmol. 34(8):755-764. |
|
|
Lima FPA, Tecchio LT, Ferreira LA, Magarifuchi M, Machado RG (2010). Evaluation of the intraocular pressure behavior in patients with assimetric primary open-angle glaucoma submitted to ibopamine provocative test. Rev. Bras. Oftalmol. 69(3):165-169. |
|
|
Minwen Z, Wei W, Wenbin H, Xiulan Z (2014). Diabetes mellitus as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. PloS one 9(8):1827-31. |
|
|
Mitchell P, Lee AJ, Rochtchina E, Wang JJ (2004). Open-angle glaucoma and systemic hypertension: the blue mountains eye study. J. Glaucoma. 13(4):319-326. |
|
|
Mitchell P, Smith W, Attebo K, Healey PR (1996). Prevalence of open-angle glaucoma in Australia. The Blue Mountains Eye Study. Ophthalmology 103(10):1661-1669. |
|
|
Newman-Casey PA, Robin AL, Blachley T, Farris K, Heisler M, Resnicow K, Lee PP (2015). The Most Common Barriers to Glaucoma Medication Adherence: A Cross-Sectional Survey. Ophthalmology 122(7):1308-1316. |
|
|
Okeke CO, Quigley HA, Jampel HD, Ying GS, Plyler RJ, Jiang Y (2009). Adherence with Topical Glaucoma Medication Monitored Electronically: The Travatan Dosing Aid Study. Ophthalmology 116:191-199. |
|
|
Owsley C (2011). Aging and vision. Vision Research. 51(13):1610-1622. |
|
|
Pasquale LR, Kang JH, Manson JE, Willett WC, Rosner BA, Hankinson SE (2006). Prospective study of type 2 diabetes mellitus and risk of primary open-angle glaucoma in women. Ophthalmology 113(7):1081-1086. |
|
|
Quigley HA, Broman AT (2006). The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 90(3):262-267. |
|
|
Quigley HA, West SK, Rodriguez J, Munoz B, Klein R, Snyder R (2001). The prevalence of glaucoma in a population-based study of Hispanic subjects: Proyecto VER. Arch. Ophthalmol. 119(12):1819-1826. |
|
|
Robin A, Grover DS (2011). Compliance and adherence in glaucoma management (2011). Indian J. Ophthalmol. 59(Suppl1):S93-S96. |
|
|
Sakata K, Sakata LM, Sakata VM, Santini C, Hopker LM, Bernardes R, Yabumoto C, Moreira AT (2007). Prevalence of glaucoma in a South brazilian population: Projeto Glaucoma. Invest Ophthalmol. Vis Sci. 48(11):4974-4979. |
|
|
Santos L, Campos GWS (2015). SUS Brazil: The health region as a way forward (2015). Saúde Soc. 24(2):438-446. |
|
|
Schneck ME, Haegerstrom-Portnoy G, Lott LA, Brabyn JA, Gildengorin G (2004). Low contrast vision function predicts subsequent acuity loss in an aged population: the SKI study. Vision Res. 44(20):2317-2325. |
|
|
Stillitano IG, Lima MGd, Ribeiro MP, Cabral J, Brandt CT (2005). Economic impact of eyedrop cost in glaucoma treatment. Arq. Bras. Oftalmol. 68(1):79-84. |
|
|
Sun J, Zhou X, Kang Y, Yan L, Sun, X, Sui, H,Yuan, H. (2012). Prevalence and risk factors for primary open-angle glaucoma in a rural northeast China population: a population-based survey in Bin County, Harbin. Eye (Lond). 26(2):283-291. |
|
|
Sun X, Xu CS, Chadha N, Chen A, Liu J (2015). Marijuana for Glaucoma: A Recipe for Disaster or Treatment? The Yale J. Biol. Med. 88(3):265-269. |
|
|
SUS Open University (UNA-SUS/UFMA). Glaucoma: SUS records 3 million calls in more than eight years and investment grows more than 300 times. |
|
|
Susanna R, De Moraes CG, Cioffi GA, Ritch R (2015). Why do people (still) go blind from glaucoma? Translational vision science & technology. 4(2):1-12. |
|
|
Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY (2014). Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 121(11):2081-2090. |
|
|
Thomas R (2012). Glaucoma in developing countries. Indian J. Ophthalmol. 60(5):446-450. |
|
|
Travassos C, Viacava F, Pinheiro R, Brito A (2002). Utilization of health care services in Brazil: gender, family characteristics, and social status. Rev. Panam Salud Publica. 11(5-6):365-373. |
|
|
United Nations (2009). World Glaucoma Day WHO reports 4.5 million people affected by the disease. |
|
|
Van der Valk R, Schouten JS, Webers CA, Beckers HJ, van Amelsvoort LG, Schouten HJ (2005). The impact of a nationwide introduction of new drugs and a treatment protocol for glaucoma on the number of glaucoma surgeries. J. glaucoma. 14(3):239-242. |
|
|
Victora CG, Barreto ML, do Carmo Leal M, Monteiro CA, Schmidt MI, Paim J, Bastos FI, Almeida C, Bahia L, Travassos C, Reichenheim M, Barros FC (2011). Health conditions and health-policy innovations in Brazil: the way forward. Lancet. 377(9782):2042-2053. |
|
|
Wensor MD, McCarty CA, Stanislavsky YL, Livingston PM, Taylor HR (1998). The prevalence of glaucoma in the Melbourne Visual Impairment Project. Ophthalmology. 105(4):733-739. |
|
|
William SF, Lanxing F, Andrew JT (2014). Visual improvement following glaucoma surgery: a case report. BMC Ophthalmol. 14:162. |
|
|
World Health Organization (WHO) (2000). The use of essential drugs: third report of the WHO Expert Committee. |
|
|
World Health Organization (WHO) (2004). Glaucoma is second leading cause of blindness globally. |
|
|
World Health Organization (WHO) (2013). Universal eye health: a global action plan 2014-2019. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


