Review
ABSTRACT
Malaria remains a disease of public health concern, which is associated with high mortality and morbidity, particularly in sub-Saharan Africa. This picture is mainly due to low effectiveness of antimalarials at the community level, a scenario caused by different factors related to the availability, quality, and efficacy of antimalarials as well as the degree of the patients’ and providers’ adherence to evidence-based recommendations about malaria treatment. This review presents an overview of the problem of low community effectiveness of antimalarials in sub-Saharan Africa, with a focus on the various causes as well as potential strategies to combat the problem.
Key words: Antimalarials, sub-Saharan Africa, disease, high mortality and morbidity.
INTRODUCTION
Despite considerable progress in the fight against malaria, the disease remains a global public health problem associated with high morbidity and mortality. According to a recent report of WHO (2014), 90% of all malaria deaths in 2013 (about 528,000 fatalities) occur in the sub-Saharan Africa. Children constitute the worst affected group, with 430,000 deaths (WHO, 2014).
The widespread resistance of Plasmodium falciparum to chloroquine and sulfadoxine-pyrimethamine (SP) prompted WHO to recommend artemisinin combination therapy WHO (2001) with the aim of delaying the emergence of resistant parasites. The recommended artemisinin-based combinations include artesunate + SP, artemether + lumefantrine (AL), artesunate + mefloquine, artesunate + amodiaquine (ASAQ), and dihydroartemisinin + piperaquine WHO (2015). The global acceptance of artemisinin-based combination therapies (ACTs) as first-line antimalarial therapy has contributed immensely to the recent global sharp decline not only in malaria deaths (Eisele et al., 2012; Tambo et al., 2012; WHO, 2014), but also in malaria cases (Gosling et al., 2011). These developments occurred partly, because of a reduction in mosquito transmission of malaria infection due to suppression of the development of P. falciparum gametocytes by the drugs (Gosling et al., 2011). Non-ACT antimalarials recommended by WHO Include SP for intermittent preventive
treatment of malaria in pregnancy (IPTp) in pregnant women and infants as well as parenteral artemisinin monotherapy and quinine for severe malaria WHO (2015).
In the next few years, the most advanced malaria vaccine (RTS,S/AS01) will be available in the market (Penny et al., 2015). However, although useful, the vaccine is only moderately effective (Penny et al., 2015), and therefore, optimizing drug treatment of malaria will remain pivotal to malaria control in the foreseeable future.
It is well known that efficacy of antimalarial drugs in the ideal situation of clinical trials is much higher than their effectiveness under the real-life situation, otherwise known as community effectiveness (Krause and Sauerborn, 2000). For any drug, including antimalarial, to be effective, it has to be of good quality, prescribed in compliance with evidence-based instructions after a correct diagnosis, and taken at an appropriate dosage, for an adequate duration (Krause and Sauerborn, 2000). Accordingly, community effectiveness is determined by drug efficacy, availability, and quality, as well as physicians’ adherence and patients’ adherence.
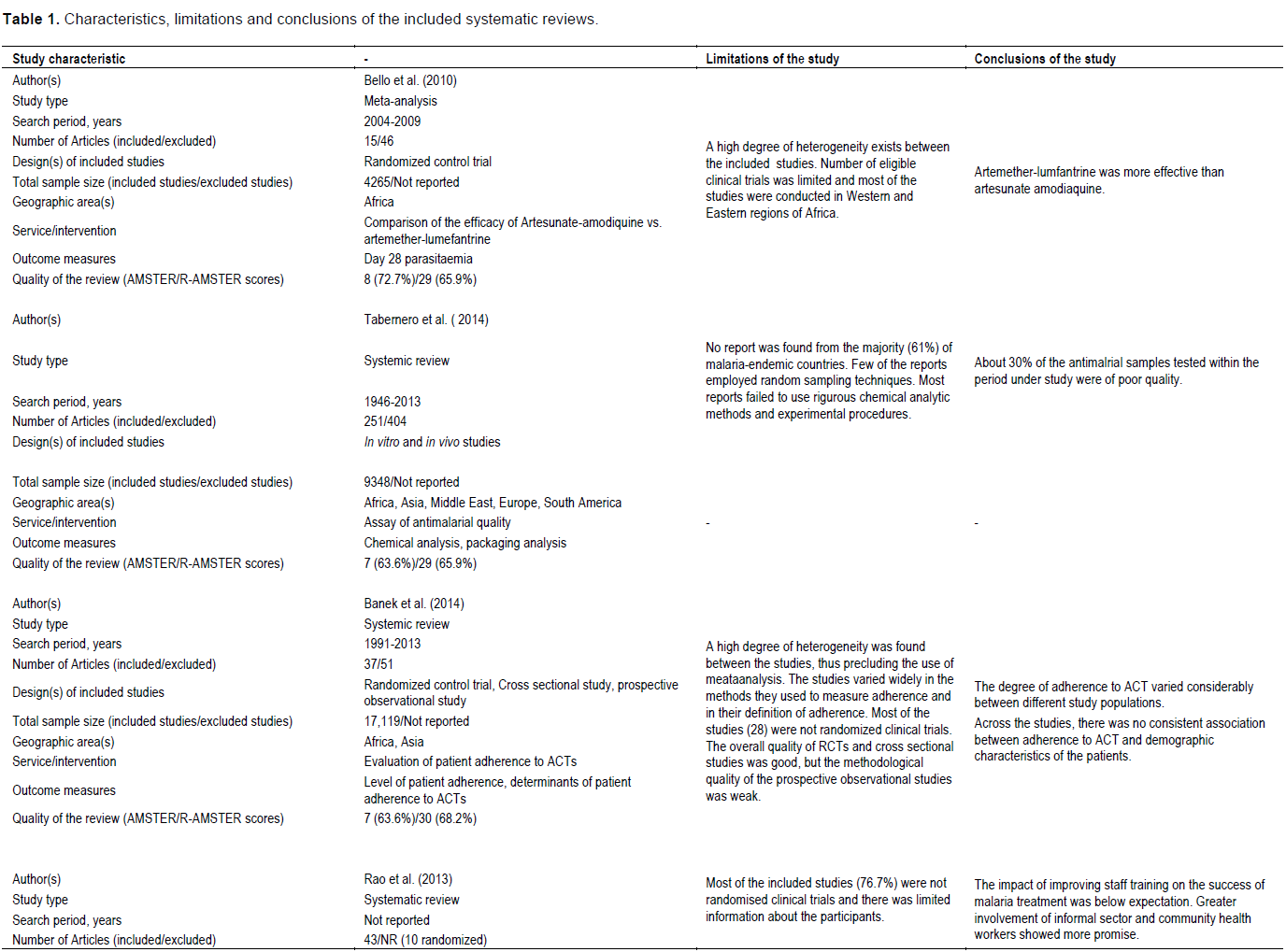
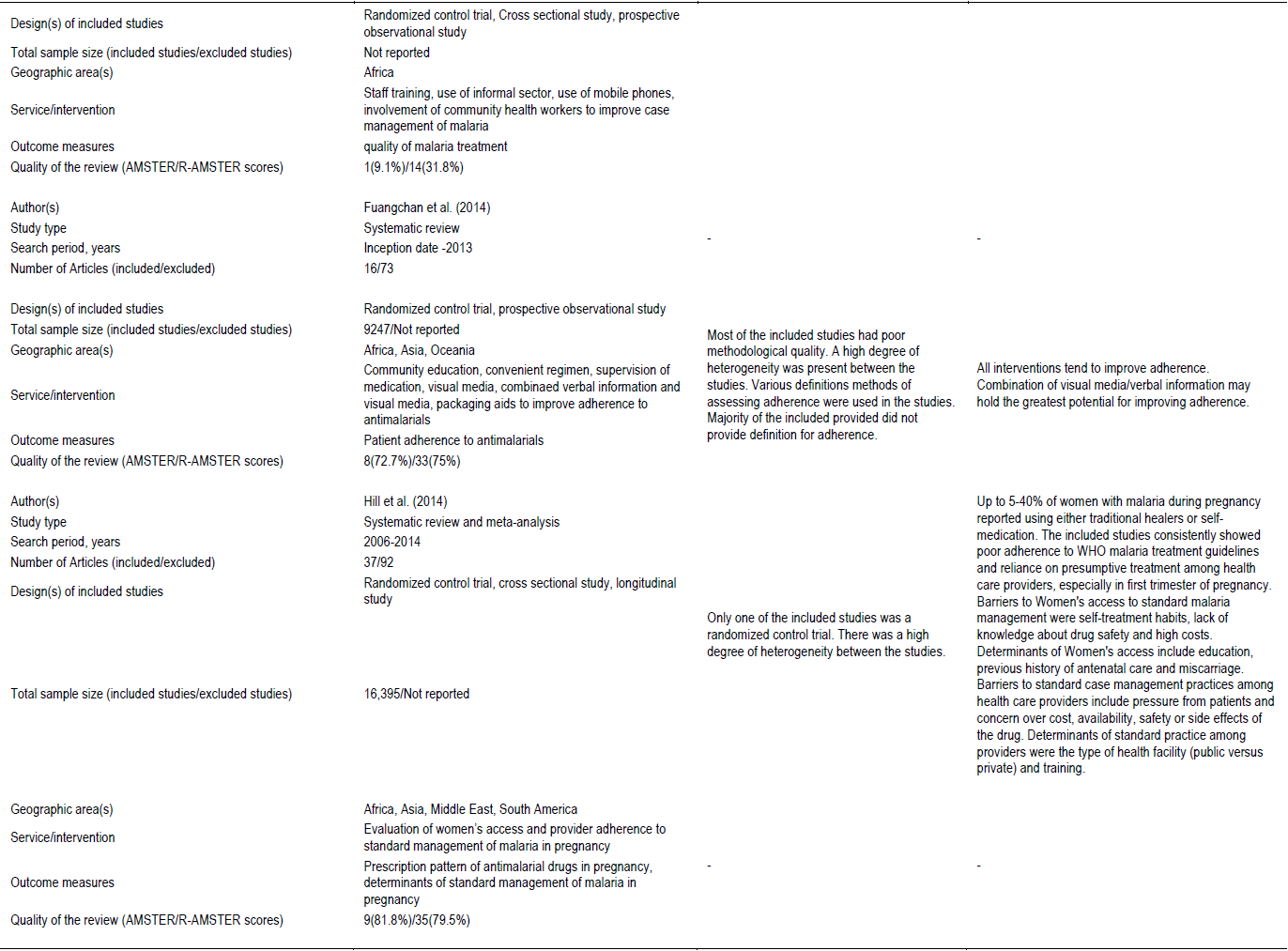
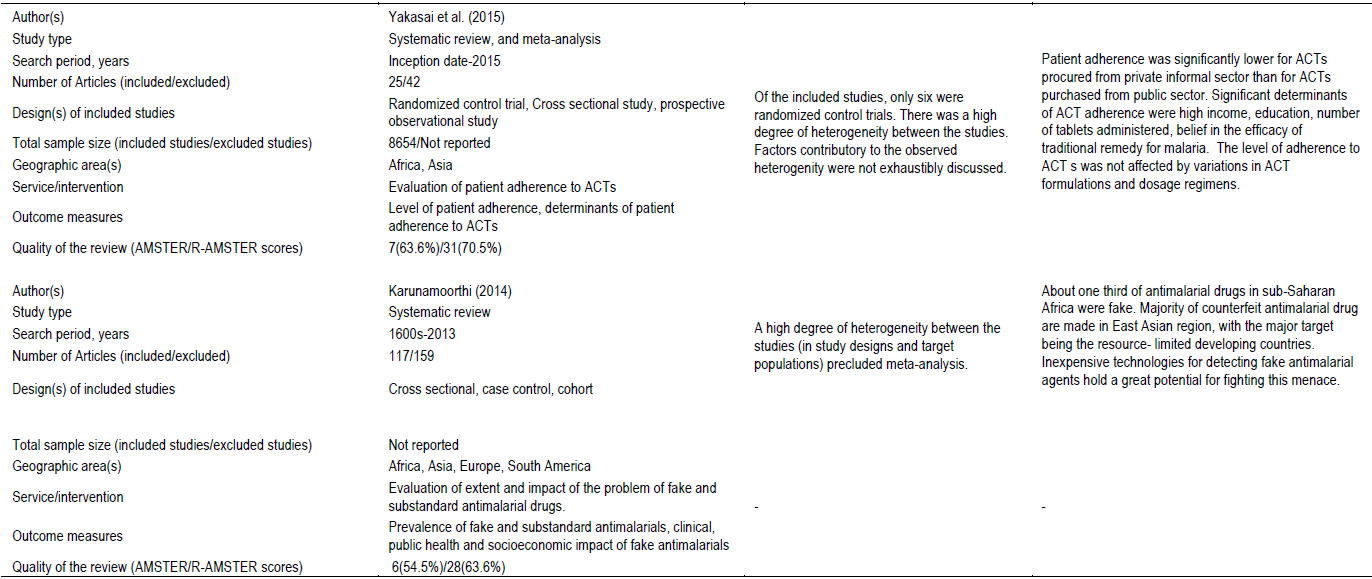
The aim of this review is to provide an updated narrative review of systematic reviews on the extent of the problem of suboptimal antimalarial community effectiveness in sub-Saharan Africa (SSA) with emphasis on the causes and possible solutions. Selected recent primary studies will also be cited to illustrate certain points. The results and methodological qualities of the included reviews are summarized in Table 1.
COMMUNITY EFFECTIVENESS OF ANTIMALARIAL DRUGS IN SSA
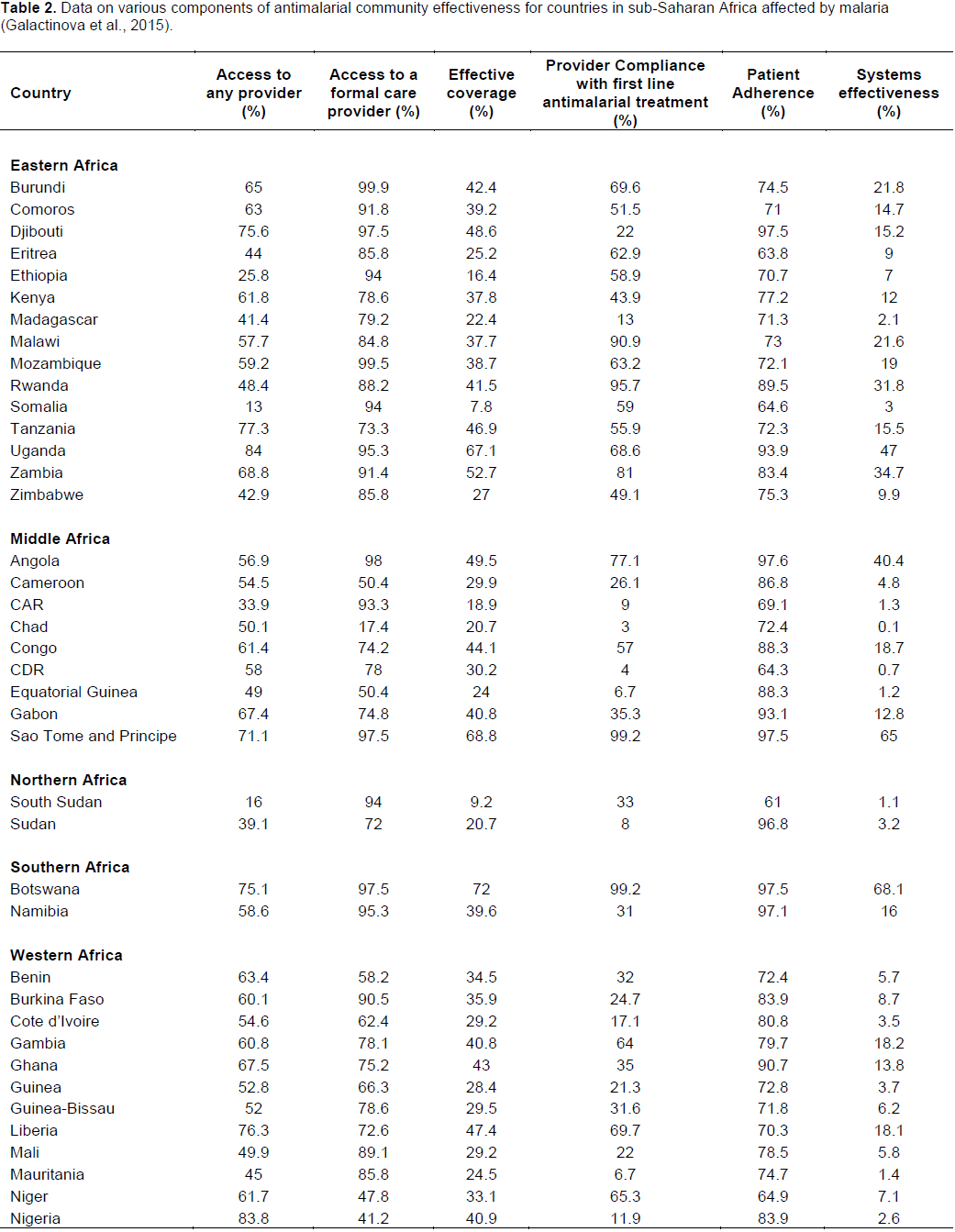
Community effectiveness of antimalarial agents can be assessed using two measures, namely systems effectiveness (Research, 2011) and effective coverage (Tanahashi, 1978; Shengelia et al., 2005). Systems effectiveness of antimalarials assesses the proportion of the community that gets cured of malaria fever after receiving drugs from formal healthcare centres (Galactionova et al., 2015). On the other hand, effective coverage, which is much wider, assesses the overall proportion of the community who are cured of malaria fever. This measure incorporates cure from self-treatment or medicines obtained from informal healthcare providers in addition to systems effectiveness (Galactionova et al., 2015).
Although artemisin in derivatives, the most frequently prescribed antimalarials, are still very effective in SSA; community effectiveness of malaria therapy is currently very low. A recent mathematical modeling based on available data (Galactionova et al., 2015) revealed a high average rate of access to malaria therapy by patients with fever (up to 60%) in the sub-Saharan African region. On the other hand, effective coverage was found to be low (about 40% on the average) in the region, ranging from 8% in Somalia to 72% in Botswana. A similar pattern was observed in systems effectiveness, which varies from 0.1% in Chad to about 68% in Botswana (Galactionova et al., 2015). The details of the data for other countries are presented in Table 2.

CHALLENGES TO ACHIEVEMENT OF OPTIMAL COMMUNITY EFFECTIVENESS OF ANTIMALARIAL DRUGS IN SSA
1. Delay in adoption of evidence-based international policies on management of malaria. For example, by the end of 2013, intermittent preventive treatment of malaria in infants was adopted by only one country in SSA (Burkina Faso) (WHO, 2014). Similarly, although WHO recommended seasonal malaria chemoprevention to 16 countries in the region, only six (Chad, Congo, Mali, Niger, Senegal, and Togo) have complied so far (WHO, 2014).
2. Poor compliance of the healthcare practitioners with first-line treatment policy: Compliance among healthcare providers represents the worst affected component of community effectiveness, with a median of 28% (Galactionova et al., 2015). This attitude has been shown to lead to antimalarial treatment failure. Countries with a low rate of compliance among healthcare givers have been observed to show a wide difference between access and effective coverage. A good example of this situation is the particular case of Nigeria, a nation with a very high access to antimalarial treatment (84%), but low effective coverage (41%), which is mainly attributable to low compliance (12%) with first-line treatment policy among its health practitioners. On the other hand, few countries, including Uganda, Botswana and Sao Tome and Principe, have high rates of both access to treatment and compliance with their respective first line treatment policies, resulting in high effective coverage (Galactionova et al., 2015). The details are shown in Table 2.
Numerous recent studies in sub-Saharan Africa have reported instances of non-compliance with the recommended national malaria treatment policy. For example, contrary to WHO recommendation, about 40% of individuals suspected to have malaria are not confirmed using laboratory test (WHO, 2014). Accordingly, individuals are still presumptively treated with antimalarials (Ezenduka et al., 2014; Isiguzo et al., 2014; Tabernero et al., 2014). Additionally, prescription of ACTs to febrile patients who tested negative for malaria parasites remains common (Hamer et al., 2007; Ndyomugyenyi et al., 2007). These two practices may lead to over treatment with ACTs and a possible increase in the risk of emergence of resistance.
In addition, recent reports in SSA have documented poor adherence of health staff to appropriate management of malaria in pregnancy (Mbonye et al., 2013; Hill et al., 2014) and non-implementation of the guidelines on IPTp (Harrison et al., 2013). Frequent prescription of artemisinin monotherapy (Builders et al., 2014; Afriyie et al., 2015; Elmannan et al., 2015; Romay-Barja et al., 2015) and lack of adoption of first-line ACT among healthcare providers in SSA have also been reported (Harrison et al., 2012).
The reported high rate of presumptive treatment of malaria by physicians in Africa is mainly attributed to lack of trust in the results of laboratory tests (Chandler et al., 2008; Rowe et al., 2009; Kyabayinze et al., 2010). Another factor contributing to poor adherence to guidelines by healthcare providers is insufficient knowledge. For example, Agbo et al. (2012) have reported poor knowledge of treatment guidelines among health staff at primary healthcare centres in Nigeria. Poor knowledge of healthcare providers about IPTp (Diala et al., 2013; Rabiu et al., 2015) and appropriate treatment of malaria in pregnancy (Rabiu et al., 2015) has also been documented.
3. Poor quality of antimalarial drugs in SSA: A recent review of 251 antimalarial quality reports from some malaria-endemic countries (Tabernero et al., 2014) has found out that about 30.1% of the antimalarials sampled were of poor quality, of which 39% were fake. However, the total picture of the problem is far from clear, due to unavailability of data from the majority of the affected nations (60%) as well as the poor methodological quality of most of the studies (Tabernero et al., 2014). In SSA, it has been estimated that up to 17% of AL purchased at informal health sectors are of poor quality. On the other hand, the estimated prevalence of fake SP is even much higher, at 33% (Tabernero et al., 2014). Most of the fake antimalarials originated in South-east Asia (Newton et al., 2011; Karunamoorthi, 2014). Renschler et al. (2015) estimated that in 2013 over 122,000 under-five children died in SSA from poor quality antimalarials.
The lucrative nature and the perceived low risk (with lenient punishment) associated with the business of making and marketing fake drugs, ineffective law enforcement and drug regulatory agencies as well as corruption are the major factors associated with the continuing existence of the problem in the sub-Saharan African region (Karunamoorthi, 2014; Tabernero et al., 2014).
4. Suboptimal effectiveness and resistance to antimalarials: In 2009, the first cases of artemisinin-resistant P. falciparum infection were observed in Cambodia (Frenk, 2010) the same region where chloroquine and SP resistance originated before it spread to Africa and other parts of the world. The resistance has been linked to a mutation in the kelch13 gene (gene ID PF3D7_1343700) (Ariey et al., 2014; Mok et al., 2015; Straimer et al., 2015). Since then, the resistant mutants have spread to other East Asian nations (WHO, 2014), but it is yet to be documented in SSA. However, there are reports of reduced effectiveness of specific ACTs in some parts of African region (Bonnet et al., 2009; Zwang et al., 2009; Group, 2011). The report of a severe case of malaria not responding to artemisinin derivatives observed in a Vietnamese man who returned from Angola is a quite disturbing development (Van Hong et al., 2014).
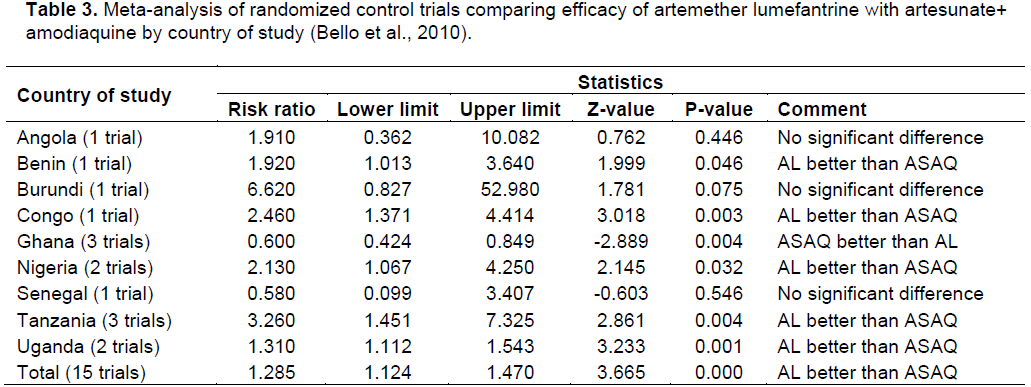
A meta-analysis by our team suggested that the efficacy of ACTs varies from one country to another (Bello et al., 2010). For example, studies from East African nations, where resistance to amodiaquine is common, suggest the superiority of AL (Table 3). On the other hand, reports from some West African nations (where amodiaquine resistance is low) indicated that ASAQ is non-inferior to AL (Happi et al., 2006; Ndiaye et al., 2009; Faye et al., 2010). Such variation in response to a particular ACT has been reported even from the same country (Bonnet et al., 2009).
One disadvantage of the use of ASAQ is the selection of mutants that are resistant to both chloroquine and amodiaquine (Frank et al., 2011; Menard et al., 2012; Van Tyne et al., 2013). It is well-known that amodiaquine undergoes cross-resistance with chloroquine (Happi et al., 2006) and resistance to amodiaquine, just like that of chloroquine, has been associated with mutations in the pfcrt and pfmdr genes (Djimdé et al., 2001; Sidhu et al., 2002). On the other hand, there is evidence suggesting that the use of AL instead of ASAQ (Alifrangis et al., 2009; Mwai et al., 2009) or even the use of concurrent multiple first-line antimalarial therapies (e.g., AL and ASAQ) as practised in some West African countries (Salissou et al., 2014) may confer an advantage in reversing chloroquine resistance.
Due to their reduced host immunity with con-sequent elevation and recurrence of parasitaemia, malnourished, especially underweight, young children, are found to be less responsive to ACTs and may require a higher dose of artemether (White, 2002; Verret et al., 2011).
5. Poor patients’ adherence to antimalarial therapy: According to a recent systematic review and meta-analysis, adherence to ACTs was significantly lower among patients who procured the drugs from patent medicine stores as compared to their counterparts who purchased the medicines from public health centres (Yakasai et al., 2015). The authors suggested that the finding might be due to the fact that patients received less qualitative instructions from patent medicine vendors. Patient adherence to ACTs also varied between different populations (Banek et al., 2014).
Self-medication with antimalarials is also common (Mussa and Gedif, 2013). In sub-Saharan Africa, medicine vendors play a role in the delivery of 15 to 85% of child healthcare products. Many of these distributors do not possess an updated licence (Palafox et al., 2014). The availability of a particular antimalarial in these shops is mainly driven by the patients demand and preference rather than the dictation of the national guidelines (Palafox et al., 2014).
Subsidy of antimalarials was first advocated by Gelband et al. (2004). The Affordable Medicines Facility for malaria (AMFm), an initiative aimed at subsiding the first-line ACTs, was created in 2008 with support from Global Fund (Gelband and Laxminarayan, 2015). However, although ACTs are subsidized or even given free in public health centres in SSA, access to the drugs is limited by frequent stockouts (Palafox et al., 2014). As a consequence, in African countries, non-ACT drugs remain more widely available and less expensive than ACT or artemisinin monotherapy (Rao et al., 2013; Palafox et al., 2014; Lussiana, 2015; Palafox et al., 2015). Accordingly, many patients, being poor and buying drugs from their pockets tend to buy the less expensive non-ACTs.
6. Poor access to antimalarials: It has been documented that up to 15 million pregnant women did not receive malaria prophylaxis in 2013 (WHO, 2014). Multiple studies have identified barriers to optimal utilization of IPTp, including out-of-pocket payments (due to lack of health insurance), lost time, stockouts, the absence of a clear policy and poor knowledge of the providers (Hill et al., 2013).
STRATEGIES FOR IMPROVING COMMUNITY EFFECTIVENESS OF ANTIMALARIAL DRUGS
Any strategy that can improve the quality or access to recommended antimalarials and increase provider adherence to malaria treatment guidelines, as well as patient adherence to the treatment, can lead to improvement of community effectiveness of the drugs.
Adoption and implementation of policies that will reduce the costs of genuine drugs (e.g., extension of the subsidy of recommended antimalarials to private health sector) will go a long way to making antimalarial counterfeiting business not attractive (Karunamoorthi, 2014). Another strategy that can help in reducing the menace is creation and enforcement of laws designed to severely punish the culprits as well as honor informants who assist in the successful conviction of those found guilty of the crime (WHO, 2005). A recent systematic review has indicated the superior effectiveness of using a multifaceted approach to tackling drug counterfeiting compared to individual interventions (El-Jardali et al., 2015). The problem of substandard and varying batch-to-batch pharmaceutical products maybe reduced through efficient internal and external quality control.
Provider adherence to antimalarial treatment guidelines, including increased implementation of IPTp, has been shown to improve following enhanced training of healthcare personnel (Mbacham et al., 2014; Mbonye et al., 2014). Also, the common practice of malaria overtreatment with ACTs may be reduced by subsidizing rapid diagnostic tests (Lussiana, 2015).
Similarly, improvement in patient adherence to anti-malarial treatment has been documented with strategies such as community education and a combination of visual media/verbal information (Fuangchan et al., 2014).
Availability of artemisinin-derived products can be optimized by expanding the subsidy to the private sector and increasing the yield of artemisinin from plant origin and supporting the semi-synthetic production of artemisinin (Fuangchan et al., 2014).
Optimal therapy of malaria can also be achieved by variation of the doses of the constituents of ACT. For instance, there is evidence that the use of an optimized fixed dose combination of ASAQ is associated with success in therapy (Sirima et al., 2009; Group, 2015), while loose non-fixed dose formulation is associated with recrudescence at day 28 of therapy (Group, 2015). Systematic reviews revealed the effect of changes in dosing on the efficacy of AL (Dose et al., 2015) and dihydroartemisinin-piperaquine (Group, 2013).
The continuing search for an effective alternative to artemisinin derivatives is highly needed due to the imminent threat of the spread of artemisinin resistance from South East Asia to other malaria-endemic nations, especially in SSA. Being a non-lucrative business, development of new drugs for parasitic infections (diseases of underdeveloped nations) is not attractive to pharmaceutical companies (Pink et al., 2005). Drug repositioning-exploration of registered drugs for new indications is a potentially cost-effective strategy for discovery of new interventions against such diseases. Using molecular docking against P. falciparum targets, our research team has applied such approach to search for new treatments for malaria with some promising results (Yunusa et al., 2015).
LIMITATIONS TO THE STUDY
There is a large amount of data on the subject area of community effectiveness of antimalarial drugs in sub-Saharan Africa. Therefore, an updated review of systematic reviews on the subject area was conducted citing selected recent primary studies to illustrate some points. A qualitative narrative approach was chosen rather than a quantitative approach to synthesizing the data due to a high degree of heterogeneity of the studies as well as the duplication of many primary studies included in the reviews. One limitation of this approach of reviewing secondary literature was that the quality of the evidence presented in the review depends on the quality of the systematic reviews. Generally, the methodological quality of the reviews was fair and comparable to that found in other reviews of systematic reviews (Burda et al., 2011).
CONCLUSION
Community effectiveness of antimalarial drugs remains low in sub-Saharan Africa. Although various factors have been documented to contribute to this picture, provider, and patient non adherence to first line treatment is the major factor that plays a key role in the development of the problem. Accordingly, community education and enhanced training of healthcare providers are pivotal in combating the problem.
ABBREVIATIONS
ACT, Artemisin-based combination therapy; AL, artemether-lumefantrine; ASAQ, artesunate + amodiaquine; IPTp, intermittent preventive treatment of malaria in pregnancy; SP, sulfadoxine-pyrimethamine; SSA, sub-Saharan Africa.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Afriyie DK, Amponsah SK, Antwi R, Nyoagbe SY, Bugyei KA (2015). Prescribing trend of antimalarial drugs at the Ghana Police Hospital. J. Infect. Dev. Ctries 9(04):409-415. |
|
|
Agbo HA, Madaki A, Envuladu E (2012). Exploring the Prevalence of Malaria and Prescribing Pattern of Antimalarial Treatment at an Urban Primary Health Care Centre. Jos J. Med. 6(2):59-62. |
|
|
Alifrangis M, Lusingu JP, Mmbando B, Dalgaard MB, Vestergaard LS, Ishengoma D, Khalil IF, Theander TG, Lemnge MM, Bygbjerg IC (2009). Five-year surveillance of molecular markers of Plasmodium falciparum antimalarial drug resistance in Korogwe District, Tanzania: accumulation of the 581G mutation in the P. falciparum dihydropteroate synthase gene. Am. J. Trop. Med. Hyg. 80(4):523-527. |
|
|
Ariey F, Witkowski B, Amaratunga C, Beghain J, Langlois AC, Khim N, Kim S, Duru V, Bouchier C, Ma L (2014). A molecular marker of artemisinin-resistant Plasmodium falciparum malaria. Nature 505(7481):50-55. |
|
|
Banek K, Lalani M, Staedke SG, Chandramohan D (2014). Adherence to artemisinin-based combination therapy for the treatment of malaria: a systematic review of the evidence. Malar. J. 13(1):7. |
|
|
Bello SO, Chika A, AbdulGafar JO (2010). Artesunate plus Amodiaquine (AS+ AQ) versus Artemether-Lumefantrine (AL) for the treatment of uncomplicated Plasmodium falciparum malaria in sub-Saharan Africa-a meta-analysis. Afr. J. Infect. Dis. 4(2):20-28. |
|
|
Bonnet M, Broek Ivd, van Herp M, Urrutia P, van Overmeir C, Kyomuhendo J, Ndosimao CN, Ashley E, Guthmann J-P (2009). Varying efficacy of artesunate+ amodiaquine and artesunate+ sulphadoxine-pyrimethamine for the treatment of uncomplicated falciparum malaria in the Democratic Republic of Congo: a report of two in-vivo studies. Malar. J. 8(1):192. |
|
|
Builders MI, Degge H, Peter JY, Ogbole E (2014). Prescription pattern of antimalarial drugs in a Teaching Hospital in Nigeria. Br. Biomed. Bull. 2(1):267-276. |
|
|
Burda BU, Norris SL, Holmer HK, Ogden LA, Smith ME (2011). Quality varies across clinical practice guidelines for mammography screening in women aged 40-49 years as assessed by AGREE and AMSTAR instruments. J. Clin. Epidemiol. 64(9):968-76. |
|
|
Chandler CI, Mwangi R, Mbakilwa H, Olomi R, Whitty CJ, Reyburn H (2008). Malaria overdiagnosis: is patient pressure the problem? Health policy Plan. 23(3):170-178. |
|
|
Diala CC, Pennas T, Marin C, Belay KA (2013). Perceptions of intermittent preventive treatment of malaria in pregnancy (IPTp) and barriers to adherence in Nasarawa and Cross River States in Nigeria. Malar. J. 12(1):1-16. |
|
|
Djimdé A, Doumbo OK, Cortese JF, Kayentao K, Doumbo S, Diourté Y, Coulibaly D, Dicko A, Su X-z, Nomura T (2001). A molecular marker for chloroquine-resistant falciparum malaria. N. Engl. J. Med. 344(4):257-263. |
|
|
Dose WARNWA, Group IS (2015). The effect of dose on the antimalarial efficacy of artemether–lumefantrine: a systematic review and pooled analysis of individual patient data. Lancet Infect. Dis. 15(6):692-702. |
|
|
Eisele T, Larsen D, Walker N, Cibulskis R, Yukich J, Zikusooka C (2012). Estimates of child deaths prevented from malaria prevention scale-up in Africa 2001–2010. Malar. J. 11:93. |
|
|
El-Jardali F, Akl EA, Fadlallah R, Oliver S, Saleh N, El-Bawab L, Rizk R, Farha A, Hamra R (2015). Interventions to combat or prevent drug counterfeiting: a systematic review. BMJ open 5(3):e006290. |
|
|
Elmannan AA, Elmardi KA, Idris YA, Spector JM, Ali NA, Malik EM (2015). Anti-malarial prescribing practices in Sudan eight years after introduction of artemisinin-based combination therapies and implications for development of drug resistance. BMC Pharmacol. Toxicol. 16(1):3. |
|
|
Ezenduka CC, Okonta MJ, Esimone CO (2014). Adherence to treatment guidelines for uncomplicated malaria at two public health facilities in Nigeria; Implications for the 'test and treat'policy of malaria case management. J. Pharm. Policy Pract. 7(1):15. |
|
|
Faye B, Offianan AT, Ndiaye JL, Tine RC, Touré W, Djoman K, Sylla K, Ndiaye PS, Penali L, Gaye O (2010). Efficacy and tolerability of artesunateâ€amodiaquine (Camoquin plus®) versus artemetherâ€lumefantrine (Coartem®) against uncomplicated Plasmodium falciparum malaria: multisite trial in Senegal and Ivory Coast. Trop. Med. Int. Health 15(5):608-613. |
|
|
Frank M, Lehners N, Mayengue PI, Gabor J, Dal-Bianco M, Kombila DU, Ngoma GM, Supan C, Lell B, Ntoumi F (2011). A thirteen-year analysis of Plasmodium falciparum populations reveals high conservation of the mutant pfcrt haplotype despite the withdrawal of chloroquine from national treatment guidelines in Gabon. Malar. J. 10(1):304. |
|
|
Frenk J (2010). The global health system: strengthening national health systems as the next step for global progress. PLos Med. 7(1):e1000089. |
|
|
Fuangchan A, Dhippayom T, Kongkaew C (2014). Intervention to promote patients' adherence to antimalarial medication: a systematic review. Am. J. Trop. Med. Hyg. 90(1):11-19. |
|
|
Galactionova K, Tediosi F, de Savigny D, Smith T, Tanner M (2015). Effective Coverage and Systems Effectiveness for Malaria Case Management in Sub-Saharan African Countries. PloS one 10(5):e0127818. |
|
|
Gelband H, Laxminarayan R (2015). Tackling antimicrobial resistance at global and local scales. Trends Microbiol. 23(9):524-526. |
|
|
Gelband H, Panosian C, Arrow KJ (2004). Saving Lives, Buying Time: Economics of Malaria Drugs in an Age of Resistance. edn. National Academies Press. |
|
|
Gosling R, Okell L, Mosha J, Chandramohan D (2011). The role of antimalarial treatment in the elimination of malaria. Clin. Microbiol. Infect. 17(11):1617-1623. |
|
|
Group AS (2015). The effect of dosing strategies on the therapeutic efficacy of artesunate-amodiaquine for uncomplicated malaria: a meta-analysis of individual patient data. BMC Med. 13(1):66. |
|
|
Group DS (2013). The Effect of Dosing Regimens on the Antimalarial Efficacy of Dihydroartemisinin-Piperaquine: A Pooled Analysis of Individual Patient Data. PLoS Med. 10(12):1-17. |
|
|
Group FA-BCS (2011). A head-to-head comparison of four artemisinin-based combinations for treating uncomplicated malaria in African children: a randomized trial. PLoS Med. 8(11):e1001119. |
|
|
Hamer DH, Ndhlovu M, Zurovac D, Fox M, Yeboah-Antwi K, Chanda P, Sipilinyambe N, Simon JL, Snow RW (2007). Improved diagnostic testing and malaria treatment practices in Zambia. JAMA 297(20):2227-2231. |
|
|
Happi C, Gbotosho G, Folarin O, Bolaji O, Sowunmi A, Kyle D, Milhous W, Wirth D, Oduola A (2006). Association between mutations in plasmodium falciparum chloroquine resistance transporter and p. falciparum multidrug resistance 1 genes and in vivo amodiaquine resistance in p. falciparum malaria–infected children in Nigeria. Am. J. Trop. Med. Hyg. 75(1):155-161. |
|
|
Harrison N, Olufunlayo T, Agomo C (2012). Utilization of the current national antimalarial treatment guidelines among doctors in army hospitals in Lagos, Nigeria. Open J. Prev. Med. 2(3):390-393. |
|
|
Harrison NE, Olufunlayo TF, Odunukwe NN (2013). Prescription of intermittent preventive therapy (IPTp) among doctors practicing in an army hospital in Lagos, Nigeria. Open J. Prev. Med. 3(2):258-261. |
|
|
Hill J, D'Mello-Guyett L, Hoyt J, van Eijk AM, ter Kuile FO, Webster J (2014). Women's Access and Provider Practices for the Case Management of Malaria during Pregnancy: A Systematic Review and Meta-Analysis. PLoS Med. 11(8):e1001688. |
|
|
Hill J, Hoyt J, van Eijk AM, D'Mello-Guyett L, ter Kuile FO, Steketee R, Smith H, Webster J (2013). Factors affecting the delivery, access, and use of interventions to prevent malaria in pregnancy in sub-Saharan Africa: a systematic review and meta-analysis. PLoS Med. 10(7):e1001488. |
|
|
Isiguzo C, Anyanti J, Ujuju C, Nwokolo E, De La Cruz A, Schatzkin E, Modrek S, Montagu D, Liu J (2014). Presumptive treatment of malaria from formal and informal drug vendors in Nigeria. PloS one 9(10):e110361. |
|
|
Karunamoorthi K (2014). The counterfeit anti-malarial is a crime against humanity: a systematic review of the scientific evidence. Malar. J. 13(1):209-209. |
|
|
Krause G, Sauerborn R (2000). Comprehensive community effectiveness of health care. A study of malaria treatment in children and adults in rural Burkina Faso. Ann. Trop. Paediatr: Int. Child Health 20(4):273-282. |
|
|
Kyabayinze DJ, Asiimwe C, Nakanjako D, Nabakooza J, Counihan H, Tibenderana JK (2010). Research Use of RDTs to improve malaria diagnosis and fever case management at primary health care facilities in Uganda. Malar. J. 9(1):200. |
|
|
Lussiana C (2015). Towards subsidized malaria rapid diagnostic tests. Lessons learned from the global subsidy of artemisinin-based combination therapies: a review. Health Policy plan.1:12. |
|
|
Mbacham WF, Mangham-Jefferies L, Cundill B, Achonduh OA, Chandler CI, Ambebila JN, Nkwescheu A, Forsah-Achu D, Ndiforchu V, Tchekountouo O (2014). Basic or enhanced clinician training to improve adherence to malaria treatment guidelines: a cluster-randomised trial in two areas of Cameroon. Lancet Glob. Health 2(6):e346-e358. |
|
|
Mbonye AK, Birungi J, Yanow S, Magnussen P (2013). Prescription patterns and drug use among pregnant women with febrile Illnesses in Uganda: A survey in out-patient clinics. BMC Infect. Dis. 13(1):237. |
|
|
Mbonye MK, Burnett SM, Burua A, Colebunders R, Crozier I, Kinoti SN, Ronald A, Naikoba S, Rubashembusya T, Willis KS (2014). Effect of integrated capacity-building interventions on malaria case management by health professionals in Uganda: A mixed design study with pre/post and cluster randomized trial components. PloS one 9(1):e84945. |
|
|
Menard S, Morlais I, Tahar R, Sayang C, Mayengue PI, Iriart X, Benoit-Vical F, Lemen B, Magnaval JF, Awono-Ambene P (2012). Molecular monitoring of Plasmodium falciparum drug susceptibility at the time of the introduction of artemisinin-based combination therapy in Yaounde, Cameroon: implications for the future. Malar. J. 11:113. |
|
|
Mok S, Ashley EA, Ferreira PE, Zhu L, Lin Z, Yeo T, Chotivanich K, Imwong M, Pukrittayakamee S, Dhorda M (2015). Population transcriptomics of human malaria parasites reveals the mechanism of artemisinin resistance. Science 347(6220):431-435. |
|
|
Mussa S, Gedif T (2013). Antimalarial Drug Use Pattern in Pawe Special Woreda, North West Ethiopia: A Community Based Survey. Ethiop. Pharm. J. 29(2):121-136. |
|
|
Mwai L, Ochong E, Abdirahman A, Kiara SM, Ward S, Kokwaro G, Sasi P, Marsh K, Borrmann S, Mackinnon M (2009). Chloroquine resistance before and after its withdrawal in Kenya. Malar. J. 8(1):106. |
|
|
Ndiaye JL, Randrianarivelojosia M, Sagara I, Brasseur P, Ndiaye I, Faye B, Randrianasolo L, Ratsimbasoa A, Forlemu D, Moor VA (2009). Randomized, multicentre assessment of the efficacy and safety of ASAQ–a fixed-dose artesunate-amodiaquine combination therapy in the treatment of uncomplicated Plasmodium falciparum malaria. Malar. J. 8(1):125. |
|
|
Ndyomugyenyi R, Magnussen P, Clarke S (2007). Malaria treatment-seeking behaviour and drug prescription practices in an area of low transmission in Uganda: implications for prevention and control. Trans. R. Soc. Trop. Med. Hyg. 101(3):209-215. |
|
|
Newton PN, Green MD, Mildenhall DC, Plançon A, Nettey H, Nyadong L, Hostetler DM, Swamidoss I, Harris GA, Powell K (2011). Poor quality vital anti-malarials in Africa-an urgent neglected public health priority. Malar. J. 10:352. |
|
|
Palafox B, Patouillard E, Tougher S, Goodman C, Hanson K, Kleinschmidt I, Rueda ST, Kiefer S, O'Connell KA, Zinsou C (2014). Understanding private sector antimalarial distribution chains: a cross-sectional mixed methods study in six malaria-endemic countries. PloS one 9(4):e93763. |
|
|
Palafox B, Patouillard E, Tougher S, Goodman C, Hanson K, Kleinschmidt I, Rueda ST, Kiefer S, O'Connell K, Zinsou C (2015). Prices and mark-ups on antimalarials: evidence from nationally representative studies in six malaria-endemic countries. Health Policy Plan. 1: 1-13. |
|
|
Penny MA, Galactionova K, Tarantino M, Tanner M, Smith TA (2015). The public health impact of malaria vaccine RTS, S in malaria endemic Africa: country-specific predictions using 18 month follow-up Phase III data and simulation models. BMC Med. 13(1):170. |
|
|
Pink R, Hudson A, Mouriès M-A, Bendig M (2005). Opportunities and challenges in antiparasitic drug discovery. Nat. Rev. Drug Discov. 4(9):727-740. |
|
|
Rabiu KA, Davies NO, Nzeribe-Abangwu UO, Adewunmi AA, Akinlusi FM, Akinola OI, Ogundele SO (2015). Malaria prevention and treatment in pregnancy: Survey of current practice among private medical practitioners in Lagos, Nigeria. Trop. Doct. 45(1):6-11. |
|
|
Rao VB, Schellenberg D, Ghani AC (2013). Overcoming health systems barriers to successful malaria treatment. Trends Parasitol. 29(4):164-180. |
|
|
Renschler JP, Walters K, Newton PN, Laxminarayan R (2015). Estimated Under-Five Deaths Associated with Poor-Quality Antimalarials in Sub-Saharan Africa. Am. J. Trop. Med. Hyg. 92(6 Suppl):119-126. |
|
|
Research mCGoHSaO (2011). A Research Agenda for Malaria Eradication: Health systems and operational research. PLoS Med. 8:e1000397. |
|
|
Romay-Barja M, Jarrin I, Ncogo P, Nseng G, Sagrado MJ, Santana-Morales MA, Aparcio P, Valladares B, Riloha M, Benito A (2015). Rural-Urban Differences in Household Treatment-Seeking Behaviour for Suspected Malaria in Children at Bata District, Equatorial Guinea. PloS one 10(8):e0135887. |
|
|
Rowe AK, De Leon G, Mihigo J (2009). Quality of malaria case management at outpatient health facilities in Angola. Malar. J. 8(1):275. |
|
|
Salissou A, Zamanka H, Biyghe Binze B, Rivière T, Tichit M, Ibrahim ML, Fandeur T (2014). Low prevalence of Pfcrt resistance alleles among patients with uncomplicated Falciparum malaria in Niger six years after chloroquine withdrawal. Malar. Res. Treat. 2014:614190. |
|
|
Shengelia B, Tandon A, Adams OB, Murray CJ (2005). Access, utilization, quality, and effective coverage: An integrated conceptual framework and measurement strategy. Soc. Sci. Med. 61(1):97-109. |
|
|
Sidhu ABS, Verdier-Pinard D, Fidock DA (2002). Chloroquine resistance in Plasmodium falciparum malaria parasites conferred by pfcrt mutations. Science 298(5591):210-213. |
|
|
Sirima SB, Tiono AB, Gansané A, Diarra A, Ouédraogo A, Konaté AT, Kiechel JR, Morgan CC, Olliaro PL, Taylor WR (2009). The efficacy and safety of a new fixed-dose combination of amodiaquine and artesunate in young African children with acute uncomplicated Plasmodium falciparum. Malar. J. 8(1):48. |
|
|
Straimer J, Gnädig NF, Witkowski B, Amaratunga C, Duru V, Ramadani AP, Dacheux M, Khim N, Zhang L, Lam S (2015). K13-propeller mutations confer artemisinin resistance in Plasmodium falciparum clinical isolates. Science 347(6220):428-431. |
|
|
Tabernero P, Fernández FM, Green M, Guerin PJ, Newton PN (2014). Mind the gaps-the epidemiology of poor-quality anti-malarials in the malarious world-analysis of the WorldWide Antimalarial Resistance Network database. Malar. J. 13:139. |
|
|
Tambo E, Adedeji A, Huang F, Chen J, Zhou S, Tang L (2012). Scaling up impact of malaria control programmes: a tale of events in Sub-Saharan Africa and Peoples Republic of China. Infect. Dis. Poverty 1:1-15. |
|
|
Tanahashi T (1978). Health service coverage and its evaluation. Bull. World Health Organ. 56:295-303. |
|
|
Tanner M, Vlassoff C (1998). Treatment-seeking behaviour for malaria: a typology based on endemicity and gender. Soc. Sci. Med. 46:523-532. |
|
|
Van Hong N, Amambua-Ngwa A, Tuan NQ, Cuong DD, Giang NTH, Van Dung N, Tinh TT, Van Tien N, Phuc BQ, Duong TT (2014). Severe malaria not responsive to artemisinin derivatives in man returning from Angola to Vietnam. Emerg. Infect. Dis. 20(7):1207. |
|
|
Van Tyne D, Dieye B, Valim C, Daniels RF, Sène PD, Lukens AK, Ndiaye M, Bei AK, Ndiaye YD, Hamilton EJ (2013). Changes in drug sensitivity and anti-malarial drug resistance mutations over time among Plasmodium falciparum parasites in Senegal. Malar. J. 12:441. |
|
|
Verret WJ, Arinaitwe E, Wanzira H, Bigira V, Kakuru A, Kamya M, Tappero JW, Sandison T, Dorsey G (2011). Effect of nutritional status on response to treatment with artemisinin-based combination therapy in young Ugandan children with malaria. Antimicrob. Agents Chemother. 55(6):2629-2635. |
|
|
White NJ (2002). The assessment of antimalarial drug efficacy. Trends Parasitol. 18(10):458-464. |
|
|
World Health Organization (WHO) (2001). Antimalarial drug combination therapy. Geneva: World Health Organisation. |
|
|
World Health Organization (WHO) (2005). Combating counterfeit drugs: a concept paper for effective international collaboration. Geneva: World Health Organization. |
|
|
World Health Organization (WHO) (2015). Guidelines for the treatment of malaria. Geneva. Report no. 9241549122 |
|
|
World Health Organization (WHO) (2014). World malaria report 2014. Geneva: World Health Organization. |
|
|
Yakasai AM, Hamza M, Dalhat MM, Bello M, Gadanya MA, Yaqub ZM, Ibrahim DA, Hassan-Hanga F (2015). Adherence to Artemisinin-Based Combination Therapy for the Treatment of Uncomplicated Malaria: A Systematic Review and Meta-Analysis. J. Trop. Med. 2015:189232. |
|
|
Yunusa A, Bello SO, Chika A (2015). Computational drug re-positioning: An approach to discover novel antimalarials. Int. J. Latest Res. Sci. Technol. 4(2):119-127. |
|
|
Zwang J, Olliaro P, Barennes H, Bonnet M, Brasseur P, Bukirwa H, Cohuet S, D'Alessandro U, Djimdé A, Karema C (2009). Efficacy of artesunate-amodiaquine for treating uncomplicated falciparum malaria in sub-Saharan Africa: a multi-centre analysis. Malar. J. 8(1):203. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


