Full Length Research Paper

ABSTRACT
In the elderly population, increased predisposition to chronic diseases and consequent use of various medications increases the chances of using a potentially inappropriate drug therapy. The purpose of this review was to analyze research that uses tools to study potentially inappropriate drug therapy through the strengthening the reporting of observational studies in epidemiology (STROBE) initiative. A systematic review was undertaken between February and March, 2013. The studies were selected from different combinations of the Medicine's controlled vocabulary thesaurus (MESH) terms - “aged,” “elderly,” “inappropriate prescribing,” and “drug utilization” in English, Spanish and Portuguese, in the Literatura Latino-Americana e do Caribe em Ciências da Saúde, PubMed, Scopus, and Web of Science databases. The papers that satisfied the inclusion criteria for data extraction were examined regarding the following variables: country, sample size, duration, type of study, practice scenario, study limitations and fulfillment of the items proposed by the STROBE initiative. At the end of the selection process, 119 articles met the specific criteria. The US had the highest number of publications in this area. The samples observed were heterogeneous, ranging from patient to database samples, and most studies were cross-sectional. The most frequently used study practice scenarios were hospitals or outpatient clinics. No article completely met the STROBE criteria. It was found that potentially inappropriate drug therapy is studied primarily in developed countries, which reinforces the need for further studies in developing countries. These findings should guide future research in this subject area, providing a more complete approach on aspects related to the use of medications by this specific population.
Key words: Potentially inappropriate drug therapy, inappropriate prescribing, elderly, study quality assessment.
INTRODUCTION
The aging process produces physiological and pathological alterations that increase the predisposition to chronic diseases and consequent use of various medications. This increased consumption of medication raises the odds of the elderly population using five or more drugs (polypharmacy), which increases the occurrence of problems related to the use of medication (Ribeiro et al., 2005; Soares et al., 2011). For this reason, pharmacotherapy for the elderly is challenging, especially if potentially inappropriate drug therapy (PIDT) is prescribed, as this increases health risks (Gallagher et al., 2007).
Medication is potentially inappropriate when its risks outweigh its benefits (Beers et al., 1991; Gallagher et al., 2008). Notably, elderly patients consume three times more medications than young adults in industrialized countries. According to Brekke et al. (2008), 10 to 20% of hospital admissions among elderly people are due to PIDT use. This is because elderly persons using PIDT are 1.8 to 1.9 times more likely to be hospitalized (Albert et al., 2010).
Additionally, there is worldwide discussion about whether the standards used in the prescription of pharmacotherapy in older people are inappropriate (Iyer et al., 2008). For example, a study conducted in the south of Ireland with 1.329 patients over 65 years of age, with an average of five drugs per patient, identified 632 prescriptions containing PIDT (Albert et al., 2010). Laroche et al. (2007) showed that the incidence of damage caused by medication was 20.4% among patients with PIDT, compared to 16.4% for patients who use only medications appropriate for the elderly.
Concerns regarding the harmful effects of the use of medication by the elderly led health professionals, such as pharmacists and physicians, to develop and implement various methods and tools to identify PIDT prescription patterns (Ribeiro et al., 2005). Therefore, the adequacy of these techniques should be evaluated by explicit and implicit methods, and the tools validated to reduce PIDT prescription (Iyer et al., 2008; Forsetlund et al., 2011).
Some revisions debate these instruments, but there are few published systematic reviews assessing the quality of studies that use tools to evaluate PIDT in various practice scenarios (Guaraldo et al., 2011; Dimitrow et al., 2011). The purpose of this review was to analyze research that uses tools to assess PIDT through the strengthening the reporting of observational studies in epidemiology (STROBE) initiative.
METHODOLOGY
A review of the scientific literature was performed to identify studies involving inappropriate prescriptions for elderly patients. The Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS), PubMed, Scopus and Web of Science databases were reviewed (up to January, 2013). The search strategy included the following keyword terms in various combinations: in English, “aged,” “elderly,” “inappropriate prescribing,” and “drug utilization”; in Spanish, “anciano,” “utilización de medicamentos,” and “prescripción inadecuada”; and in Portuguese, “idoso,” “medicamento inapropriado,” “medicamento inadequado,” and “uso de medicamento”. The research strategies were adapted according to the protocols of each database. The keywords were defined using the National Library of Medicine's controlled vocabulary thesaurus (MeSH). It consists of sets of descriptors, arranged in a hierarchical structure that permits searching at various levels of specificity. In addition to the MeSH terms, other non-standard terms were used to expand the search strategy. The study design followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
The subsequent screening process was performed in three stages (title, abstract, and full text screening) by two researchers (APALS and DTS); when there was disagreement, a third researcher (DPLJ) analyzed and judged the discrepancy. The measure of agreement between the two reviewers - defined as Cohen’s kappa (k) was calculated with a confidence interval of 95%. The titles and abstracts were compared using the following predefined inclusion criteria to determine the relevance of the theme: (i) the study involved the use of potentially inappropriate medication for elderly patients, and (ii) the study used a validated tool to make such an assessment.
A researcher (APALS) performed an initial selection, which excluded the titles that did not meet the inclusion criteria. The studies excluded were as follows: (i) reviews and editorials; (ii) studies not written in English, Portuguese, or Spanish; (iii) studies that did not provide the abstract or full text (even with attempts to get them by direct email to the authors); (iv) studies that evaluated only one or two classes of drugs; and (v) studies evaluating PIDT in only one or two diseases.
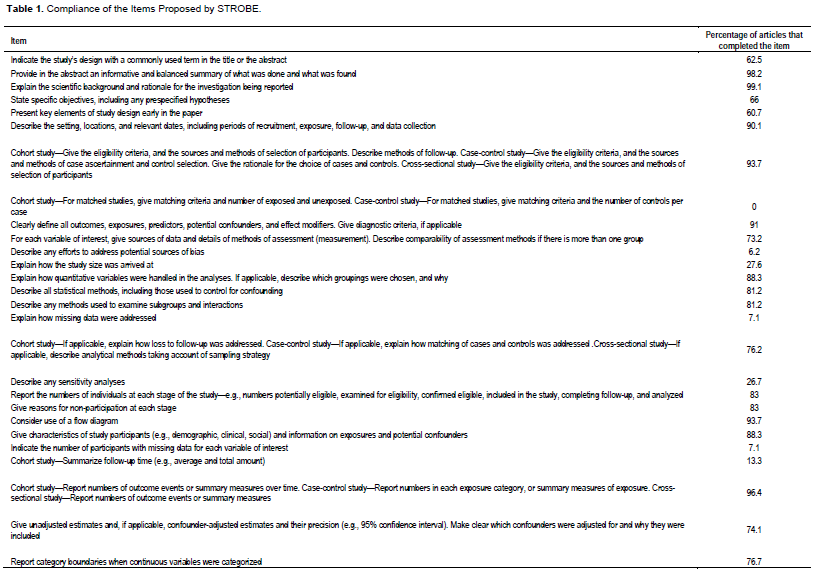
The papers that satisfied the inclusion criteria for data extraction were carefully examined regarding the following variables: country, sample size, duration, study type, practice scenario, language of publication, limitations, and fulfillment of the items proposed by the STROBE initiative. The final analysis was performed to assess the methodological rigor of the articles published in this research area; for that purpose, the STROBE tool was used (Malta et al., 2010). The tool’s 22 items were separated into 34 items to perform a more complete and accurate description of observational studies. In this review, each item fulfilled by the article was awarded one point; thus, the score could vary from 0 (0%) to 34 (100%) points.
RESULTS
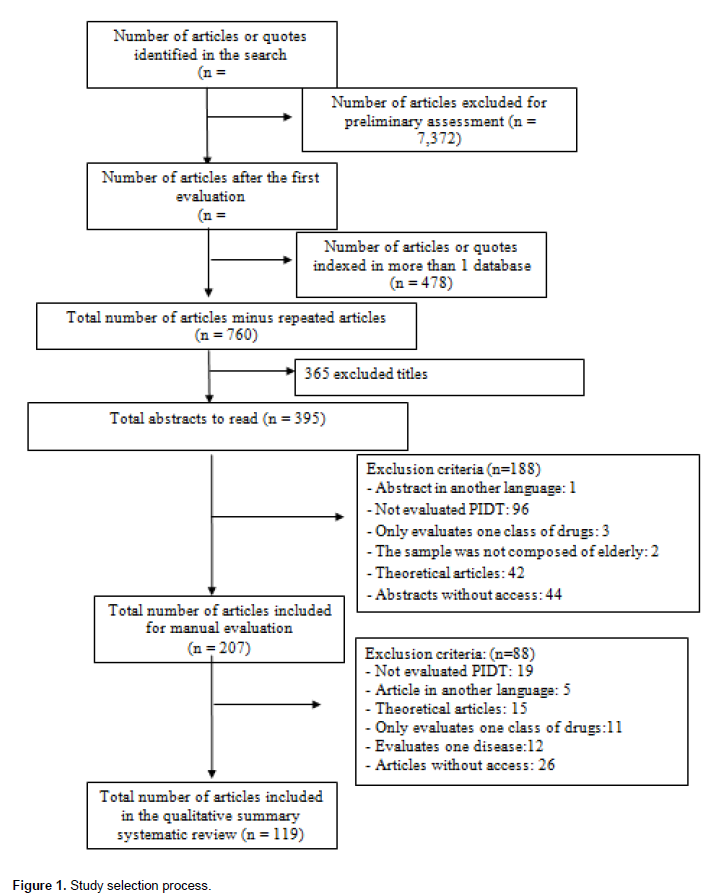
From the various combinations of keywords, 8,610 articles were found. The first evaluation was performed by one of the evaluators (APALS) who excluded 7,372 articles that did not meet at least one of the inclusion criteria. Of the remaining 1,238 articles, 478 were repeated in the databases. Thus, 760 titles were considered potentially relevant. Of these, 365 were excluded for not meeting the inclusion criteria, leaving 395 items to be evaluated according to the abstracts. In this study, 44 abstracts were not available; therefore, 351 abstracts were read and evaluated. From this evaluation, a further 144 articles were excluded for not meeting the inclusion criteria, leaving 207 articles to be read. At first, 76 articles had no free access, and 50 articles were later retrieved by the bibliographic commutation program of the Brazilian Institute of Science and Technology (IBICT-Comut). Of the articles assessed manually, 62 did not meet the inclusion criteria. At the end of the selection process, 119 articles met the specific inclusion criteria.
Figure 1 shows the progressive selection, number of articles, and reasons for exclusion at each step. The degree of agreement among the researchers was moderate for the titles (k = 0.479) and substantial for abstracts (k2 = 0.647). At all stages, the intervention of a third evaluator was necessary to resolve disagreements between the two primary researchers (Figure 1).
Of the selected studies, 40.3% were performed in Europe, 32.7% in North America, and 4.2% did not indicate the country where the research was conducted. The samples observed were heterogeneous; some studies evaluated individual patients, while other studies evaluated prescriptions in databases. Thus, the sample size varied from 30 patients in the study by Stuij et al. (2008) to 33,830,599 prescriptions in the study by Lai et al. (2009). When we grouped the different samples used in “number of reviews,” the average number of reviews (patients or prescriptions) across studies was 1,223. Three studies did not specify the sample size. The duration of the studies varied from 1 month to 9 years. Notably, 79% of the studies did not indicate or specify a study duration.
Among the studies, 32.7% were cross-sectional, 19.3% were cohort, and 19.3% did not report which methodological design was used in the study. In addition, 22.6% did not provide a complete description of the methodological design. As for the study scenario, the most frequent were hospitals or outpatient clinics, which accounted for 38.6% of the studies. In 8.4% of the studies, retirement, social security, and health plan databases were used for data collection. Only two studies were undertaken using more than one study scenario (Crotty et al., 2004; Miquel et al., 2010). Additionally, 94.9% of the studies were written in English, and 15.9% of the articles did not mention their limitations in the text. Regarding the fulfillment of the items proposed by STROBE, 49 articles met between 60 and 100% of the 34 items recommended by the initiative (Table 1).

DISCUSSION
Most of the studies included were performed in the US. This may be because the Beers criteria (most used/cited in the literature), STOPP-START criteria, Medication Appropriateness Index (MAI), Assessing Care of Vulnerable Elders (ACOVE), drug use review (DUR), HEDIS criteria, and Zhan criteria were developed there. The prevalence of studies and criteria developed in the US confirms the country as a pioneer in the clinical arena, especially regarding the evaluation of pharmacotherapy (Silva et al., 2010). Additionally, several studies were conducted in Europe, which further indicates the progress of PIDT research in developed countries compared to developing countries. Therefore, it is necessary for developing countries to increase research in this area, focusing on the effectiveness of treatments and above all, the safety of patients.
In the reviewed studies, we found a high variation in sample size, which provided a comprehensive evaluation of the tools used in different sample groups. However, two studies did not clearly describe the size of the sample surveyed (Goulding, 2004; Van der Hooft et al., 2005). In this case, two studies indicated that the lack of information on the sample could reduce the impact of the study (Holmes et al., 2009; Malta et al., 2010). Therefore, the sample in which the hypothesis is being tested should be stated and comprehensively detailed to ensure the robustness of the study.
The largest study samples consisted of retirement and health plan databases to evaluate PIDT. Despite being a viable strategy to assess the situational diagnosis of a sample, it is necessary to question the validity of the results obtained from databases such as these because the use of secondary data can mask possible selection biases. According to Guaraldo et al. (2011), an active data search can decrease the overestimation or underestimation of drug use because it is unknown whether the patient actually used the prescribed pharmacotherapy.
There was a variation of 107 months between studies. Additionally, some of the manuscripts were unclear in differentiating between the time of data collection and the study duration. Thus, in most of the articles, the real time of execution of the study is not clear, which compromises the reader’s understanding. According to von Elm et al. (2007), the author should describe the context in which the study is inserted, in addition to locations and relevant dates, including periods of recruitment, exposure, follow-up (if any), and data collection. Thus, an adequate description assists in the analysis of the results of the study so that they can be incorporated into public policies and/or large interventions, if necessary.
In this review, there were a large number of cross-sectional studies. The cross-sectional study can be used as an analytical study to evaluate hypotheses of association between exposure/characteristics and an event; they are cost-effective, easy, and fast to perform. In addition, they describe what happens to a particular group, at a particular time, and are thus important guides for decision making in the health-planning sector (Lima-Costa and Barreto, 2003). However, there are limitations when trying to identify the nature of the relationships between exposure and event in these situations. Therefore, confounding factors must be considered in this type of study, which emphasizes the need for clinical trials to evaluate the effect of PIDT in the elderly population (Hanlon et al., 2000). Approximately 42% of the studies included in the analysis either lacked methodological rigor in the description of the study design or did not mention it at all. Methodological rigor is necessary to provide sufficient detail so that the reader can understand and duplicate the methodology if they wish (Holmes et al., 2009).
Among the practice scenarios, there was a higher prevalence of studies performed with institutionalized elderly people in comparison to studies with non-institutionalized elderly. However, this prevalence exists because the criteria used for these studies have been primarily developed for evaluating the pharmacotherapy of non-institutionalized elderly patients who have different socio-demographic and clinical characteristics from institutionalized patients (Hanlon et al., 2011). Moreover, it was observed that some tools developed a priori for non-institutionalized elderly patients were used in institutions. According to Bakken et al. (2012), the application of these criteria should be carefully applied, because they can be affected by differences in study population and data source. The institutionalization of patients can facilitate the collection and evaluation of data, justifying the high number of hospital-based studies. In this sense, the applicability and reliability of these tools should be evaluated carefully through the analysis of the results obtained in their respective studies to avoid reproducing the erroneous selection of criteria.
Regarding the citation of research limitations in the text, most of the studies were in agreement with Malta and colleagues who advocate that the manuscript should describe its limitations and consider potential sources of inaccuracy (Malta et al., 2010). Further, the study should discuss the magnitude and direction of potential bias, which is essential for the reader's understanding, as well as evaluations by the article reviewers (Holmes et al., 2009; Malta et al., 2010). Fewer than half of the observational articles included in the review fulfilled 60% or more of the items proposed by STROBE. Overall, the studies included in this review had no good methodological consistency. This may be related to lack of standardization of studies and the fact that discussion on the use of PIDT has been recent. The intention of the STROBE initiative is to offer a recommendation on how to report observational studies more accurately, without making recommendations or prescriptions to the design or conduct of these studies. However, adherence to the items contributes to a more accurate report of such studies, and consequently facilitates the review of these publications by editors, reviewers, and readers (Malta et al., 2010).
In general, the results of the studies included in this review indicated high levels of PIDT. Strategies to reduce unnecessary prescriptions should be implemented to promote more appropriate use of these medications among this age group. The careful use of PIDT lists can assist with the detection of these drugs and prevent problems related to their use (Gallagher et al., 2007). In addition to identification of PIDT, it is necessary to undertake practical interventions. A study that aimed to systematically review the effects of interventions to optimize prescription found that, of the 16 studies assessed, 8 reviewed the impact of educational interventions, and of those, six showed statistically significant improvements in prescription quality. A multi-faceted approach and clearer policy guidelines are required to improve prescriptions for these vulnerable patients (Loganathan et al., 2011). Moreover, strategies shown to be effective for improving prescription outcomes include educational outreach visits (academic detailing), and interventions involving a pharmacist. Pharmacist services, such as conducting medication reviews or providing advice to general practitioners, may lead to improvements in prescription outcomes (Clyne et al., 2013).
Strengths and limitations
The study’s strength is that it was the first review to assess the methodological rigor of studies evaluating PIDT. Its limitations include the use of English, Portuguese, and Spanish keywords, which can omit important publications in different languages; this limitation is common to systematic review articles. Other keywords, such as “potential inappropriate drug therapy,” were not used. Furthermore, database restriction and the search strategy may have excluded important studies not published in the data sources used. The exclusion criteria used in this study may have also excluded relevant studies; however, it was necessary to adopt such measures, as the review’s purpose was to evaluate studies focusing on various diseases and medications. Moreover, no studies were analyzed that evaluated the omission or sub-use of medication, and studies that obtained negative results may not have been published.
Agenda for future studies
Current PIDT studies are potentially valuable because, in general, their objective is to verify PIDT prevalence in various scenarios, as well as serve as a warning to health care professionals who work with elderly patients. However, more research is needed in this area, particularly in developing countries, as it is necessary to evaluate the morbidity and mortality related to PIDT use. To reduce the limitations of PIDT studies, an active data collection search is needed, through which the reported prevalence of PIDT will be more reliable. Moreover, studies that relate the use of PIDT with outcomes such as adverse effects, hospitalizations, and deaths are rare, but are required to verify the real problems associated with using PIDTs. As noted in this review, studies evaluating interventions, such as education, have shown positive results. Thus, more studies, especially randomized clinical trials, are needed to conclude whether the interventions are indeed effective.
CONCLUSION
A discussion of the methodological rigor of studies evaluating PIDT is critical and can contribute to the wider health care discussion. This review showed that PIDT is studied mainly in developed countries, which reinforces the need for more research in developing countries. The articles included in this study focused on observing the prevalence of PIDT in various practice scenarios. Most studies were observational and fulfilled at least 40% of the items proposed by the STROBE initiative. Our results have highlighted the potential for more detailed studies about PIDT with practical implications for patient safety.
ACKNOWLEDGEMENTS
This study was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq); Fundação de Apoio à Pesquisa e à Inovação Tecnológica do Estado de Sergipe (Fapitec/SE).
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
|
Albert SM, Colombi A, Hanlon J (2010). Potentially inappropriate medications and risk of hospitalization in retirees. Drugs Aging 27(5):407-415. crossref |
||||
|
Bakken MS, Ranhoff AH, Engeland A, RuthS (2012). Inappropriate prescribing for older people admitted to an intermediate-care nursing home unit and hospital wards. Scand. J. Prim. Health Care 30(3):169-175. crossref |
||||
|
Beers MH, Ouslander JG, Rollingher I, Reuben DB, Brooks J, Beck JC (1991). Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA Division of Geriatric Medicine. Arch. Intern. Med. 151(9):1825-1832. crossref |
||||
|
Brekke M, Rognstad S, Straand J, Furu K, Gjelstad S, Bjørner T, Dalen I (2008). Pharmacologically inappropriate prescriptions for elderly patients in general practice: How common? Baseline data from The Prescription Peer Academic Detailing (Rx-PAD) study. Scand. J. Prim. Health Care 26(2):80-85. crossref |
||||
| Clyne B, Bradley MC, Smith SM, Hughes CM, Motterlini N, Clear D, McDonnell R, Williams D, Fahey T; OPTI-SCRIPT Study Team (2013). Effectiveness of medicines review with web-based pharmaceutical treatment algorithms in reducing potentially inappropriate prescribing in older people in primary care: a cluster randomized trial (OPTI-SCRIPT study protocol). Trials 13:14:72. | ||||
|
Miquel MC, Cuervo MS, Silveira ED, Machuca IS, González-Blázquez S, Errasquin BM, Cruz-Jentoft AJ (2010). Potentially inappropriate drug prescription in older subjects across health care settings. Eur. Geriatr. Med.1:9-14. crossref |
||||
|
Crotty M, Rowett D, Spurling L,Giles LC, Phillips PA (2004). Does the addition of a pharmacist transition coordinator improve evidence-based medication management and health outcomes in older adults moving from the hospital to a long-term care facility? Results of a randomized, controlled trial. Am. J. Geriatr. Pharmacother. 2(4):257-264. crossref |
||||
|
Dimitrow MS, Airaksinen MS, Kivelä SL,Lyles A, Leikola SN (2011). Comparison of prescribing criteria to evaluate the appropriateness of drug treatment in individuals aged 65 and older: a systematic review. J. Am. Geriatr. Soc. 59(8):1521-1530. crossref |
||||
|
Forsetlund L, Eike MC, Gjerberg E,Vist GE (2011). Effect of interventions to reduce potentially inappropriate use of drugs in nursing homes: a systematic review of randomised controlled trials. BMC Geriatrics 11:16. crossref |
||||
|
Gallagher P, Barry P, O'Mahony D (2007). Inappropriate prescribing in the elderly. J. Clin. Pharm. Ther. 32(2):113-121. crossref |
||||
|
Gallagher P, Ryan C, Byrne S, Kennedy J, O'Mahony D (2008). STOOP(Screening Tool of Older Person's Prescriptions) and START(Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int. J. Clin. Pharmacol. Ther. 46(2):72-83. crossref |
||||
|
Goulding MR (2004). Inappropriate medication prescribing for elderly ambulatory care patients. Arch. Intern. Med. 164:305-312. crossref |
||||
|
Guaraldo L, Cano FG, Damasceno GS,Rozenfeld S (2011). Inappropriate medication use among the elderly: a systematic review of administrative databases. BMC Geriatrics 11:79. crossref |
||||
|
Hanlon JT, Shimp LA, Semla TP (2000). Recent advances in geriatrics: drug-related problems in the elderly. Ann. Pharmacother. 34:360-365. crossref |
||||
|
Hanlon JT, Wang X, Castle NG,Stone RA, Handler SM, Semla TP, Pugh MJ, Berlowitz DR, Dysken MW (2011). Potential underuse, overuse and inappropriate use of antidepressants in older veteran nursing home patients. J. Am. Geriatr. Soc. 59(8):1412-1420. crossref |
||||
|
Holmes Jr DR, Hodgson PK, Nishimura RA, Simari RD (2009). Manuscript preparation and publication. Circulation 120:906-913. crossref |
||||
|
Iyer S, Naganathan V, McLanchlan AJ, Le Couteur DG (2008). Medication withdrawal trials in people aged 65 years and older: a systematic review. Drugs Aging 25(12):1021-1031. crossref |
||||
|
Laroche ML, Charmes JP, Nouaille Y,Picard N, Merle L (2007). Is inappropriate medication use a major cause of adverse drug reactions in the elderly? Br. J. Clin. Pharmacol. 63(2):177-186. crossref |
||||
| Lima-Costa MF, Barreto SM (2003). Types of epidemiologic studies: basic concepts and uses in the area of aging. Epidemiologia e Serviços de Saúde 12(4):189-201. | ||||
|
Loganathan M, Singh S, Franklin BD,Bottle A, Majeed A (2011). Interventions to optimise prescribing in care homes: systematic review. Age Ageing 40(2):150-162. crossref |
||||
|
Malta M, Cardoso LO, Bastos FI, Magnanini MMF, Silva CMFP (2010). Iniciativa STROBE: subsíduos para comunicação de estudos observacionais. Rev. Saúde Pública 44(3): 559-565. crossref |
||||
| Ribeiro AQ, Araújo CMC, Acurcio FA,Magalhães SMS, Chaimowicz F (2005). Quality assessment of drug use in the elderly: a review of available evaluation methods. Ciênc.saúde coletiva 10(4):1037-1045. | ||||
|
Silva DT, Santos AP, Aguiar PM, da Silva WB, Lyra Jr DP (2010). Analysis of research quality regarding pharmaceutical intervention in elderly residents of long-term care facilities: a systematic review. J. Am. Geriatr. Soc. 58(7):1404-1406. crossref |
||||
|
Soares MA, Fernandez-Llimos F, Cabrita J, Morais J (2011). Tools to evaluate potentially inappropriate prescription in the elderly: a systematic review. Acta Med. Port. 24(5):775-784. Pubmed |
||||
|
Van der Hooft CS,'t Jong GW, Dieleman JP, Verhamme KMC, Van der Cammen TJM, Stricker BHCH, Sturkenboom MCJM (2005). Inappropriate drug prescribing in older adults: the updated 2002 Beers criteria: a population-based cohort study. Br. J. Clin. Pharmacol. 60(2):137-144. crossref |
||||
|
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, for the STROBE Initiative (2007). Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335(7624):806-808. crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


