Full Length Research Paper
ABSTRACT
This work is a prospective study that aims to evaluate the vitamin D status of Moroccan women during the last trimester of their pregnancy to establish the prevalence of hypovitaminosis D. We carried out, within the Mohammed V Military Teaching Hospital (HMIMV), a six-month prospective study on the vitamin status D of 152 Moroccan women during their last gestational trimester. Maternal blood was collected at the Gynecology-Obstetrics Department during the last prenatal visit or during the delivery process. Serum assays for 25 (OH) D3, PTH, calcium, phosphorus and PAL were performed in the HMIMV Biochemistry Laboratory. A questionnaire was developed to reveal different parameters influencing vitamin status. The vitamin D deficiency rate is very high in our study sample. We found 97.37% hypovitaminosis D (<30 ng / ml) of which 9.21% in insufficiency ([20-30] ng / ml), 88.16% in deficiency (<20 ng / ml). Statistical analysis shows no correlation between age and vitamin concentration (p = 0.933). We found a negative correlation between 25 (OH) D3 and parathormone (PTH) (p = 0.016, r = - 0.194) and observed a variation of 25 (OH) D3 according to the sun, the BMI and the pigmentation of the skin although no statistical relationship has been established. There is no association between physical activity and 25 (OH) D3 concentration (p = 0.331). We recommend the implementation of corrective measures that focus on vitamin D information campaigns. The pregnant woman should be encouraged to receive adequate nutrition and a balanced diet.
Keys words: 25-hydroxy-vitamin D3, calciferol, pregnancy, hypovitaminosis D.
INTRODUCTION
Vitamin D, also known as calciferol (which etymologically means "the one that carries calcium"), is a term that applies to a set of chemically distinct secosterols, numbered from 1 to 7, all of which have antirachitic activity. Vitamins D3 and D2 are the main forms present in the human body Fugain and Jacquot (2015).
This substance results in more than 90% of the irradiation of a provitamin by ultraviolet radiation type B (UVB). Serum 25OHD level is widely considered as a marker of vitamin D nutriture, and consideration of serum 25OHD measures for the purposes of nutrient reference value development has generated notable interest. There is agreement that circulating serum 25OHD levels are currently the best available indicator of the net incoming contributions from cutaneous synthesis and total intake (foods and supplements) (Brannon et al., 2008). Thus, the serum 25OHD level may function as a biomarker of exposure; it is a reflection of the supply of vitamin D to the body and can be a useful adjunct to examining the intake level of vitamin D if the confounders and the measure's variability depending upon a range of variables are kept in mind (IOM., 2011).The vitamin D status is established only after the determination of serum 25 (OH)D. Most of the measurable 25-hydroxyvitamin in serum is 25-hydroxyvitamin D3 while 25-hydroxyvitamin D2 reaches measurable levels only in patients on vitamin D2 supplementation. Vitamin D deficiency can lead to an array of problems, most notably rickets in children and osteoporosis in adults. Many conflicting studies are now showing an association between vitamin D deficiency and cancer, cardiovascular disease, diabetes, autoimmune diseases, and depression (Stefan et al., 2019; Omeed et al., 2020). Vitamin D deficiency is associated with risk of developing peripheral arterial disease in type 2 diabetic patients (Jing et al., 2019). As an individual becomes deficient in vitamin D, intestinal calcium and phosphorous absorption decrease; serum ionized calcium levels drop, and synthesis of parathyroid hormone (PTH) is stimulated. Increased plasma PTH maintains serum calcium in the normal range by enhancing renal production of 1,25(OH)2D, increasing bone turnover, accelerating bone loss, and promoting tubular calcium reabsorption and phosphate excretion (Mulligan et al., 2010). The maternal vitamin D status, therefore, has a first-order influence on that of the fetus (Daniel et al., 2018). Numerous studies have reported associations between vitamin D deficiency during pregnancy and adverse outcomes both on maternal health and fetal development (Wagner et al., 2017). Poor maternal vitamin D status has indeed been correlated with pregnancy complications such as preeclampsia, premature birth, infants born small for gestational age and respiratory tract infections among children (Sophie et al., 2019). Our work is a prospective study that aims to evaluate the vitamin D status of Moroccan women during the last trimester of their pregnancy to establish the prevalence of hypovitaminosis D. We will highlight the existing relationships between Vitamin D status and sun exposure, dietary habits and clothing.
MATERIALS AND METHODS
Pregnant women in their last trimester of pregnancy were conveniently recruited between September 2009 through February 2010 while attending their routine antenatal care appointment at the service of gynecology and Obstetrics of the Mohammed V Military Teaching Hospital (HMIMV). Inclusion criteria were pregnancy, plans to deliver at the service of gynecology and Obstetrics, minimum age of 18 years. Exclusion criteria were multiple pregnancies, HIV infection, history of parathyroid, renal or liver diseases, chronic malabsorption syndromes or granuloma-forming disorders, age below 17 years or known (or suspected) drug or alcohol abuse. For eligible participants, an informed consent was obtained by the physician. A 5 mL blood sample was drawn during routine blood collection. Dosing results for vitamin D and other biological parameters (Parathormone, Calcium, Phosphorus, Phosphatases alcalines) have been noted. Study participants and the responsible physician completed together a questionnaire aiming at gathering socio-demographic information as well as data related to the pregnancy and lifestyle. Our final sample consisted of 152 women. Approval was provided by head of department. The Service of Clinical Biochemistry of the Mohammed V Military Teaching Hospital (HMIMV) analysed all blood samples within hours following collection: after centrifugation and serum extraction, the 25 (OH) D3 assay performed on Roche Diagnostics® Cobas e 601 Analyzer, electro-chemo-luminescence immunoassay. Hypovitaminosis D is defined as a level of 25 (OH) D <30 ng / ml. Deficiency is defined as 20-30 ng / mL (50 to 75 nmol / L), moderate deficiency for 12 to <20 ng / mL (25 to 50 nmol / L), Severe deficiency for a level <12 ng / ml (<25 nmol / L). Reference values: Calcium: 85-101 mg / L Phosphorus: 25-49 mg / L PAL: 50-136 U / L. The following data were collected: name and surname, age, weight, height, calculated body mass index (BMI), frequency of consumption of vitamin D-rich foods (For eating habits, we collected the frequency of consumption of foods rich in vitamin D and available on the Moroccan market), The presence and content of drug supplementation, the parameters of exposure to the sun (wearing protective clothing, use of sunscreens, duration and frequency of sun exposure, ...), and the practice or not of sports activities such as walking, hiking, jogging, biking, swimming, aerobic indoor dance, daily ascent and descent of stairs, period at enrolment first period (September 29st – November 30th) 2009, second period (December 1st, 2009 February 24st, 2010). Our final sample consisted of 78 for first period (maximum sunshine) and 74 for second period (minimum sunshine). Statistical analysis was provided by the SPSS statistical software version 13.01. For comparisons of quantitative variables, we used the Student’s t and ANOVA tests. The results are considered statistically significant from a value p <0.05.
RESULTS
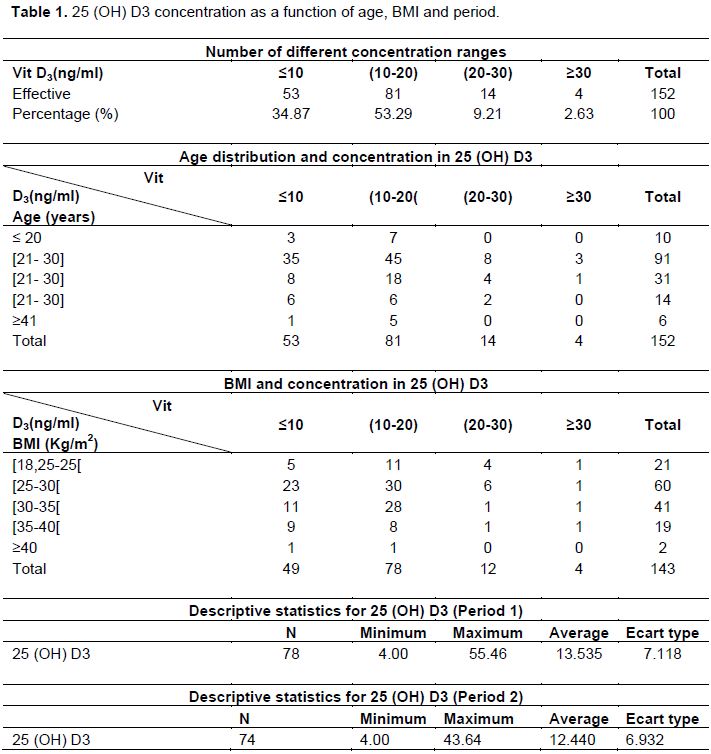
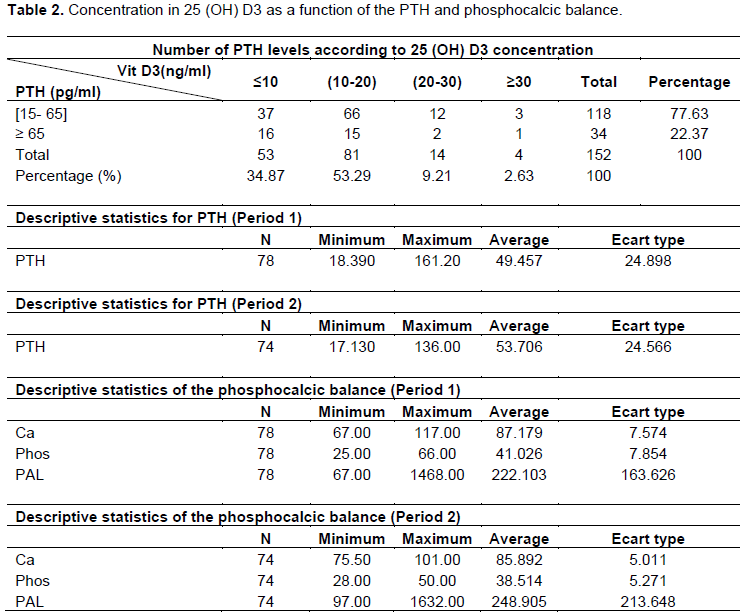
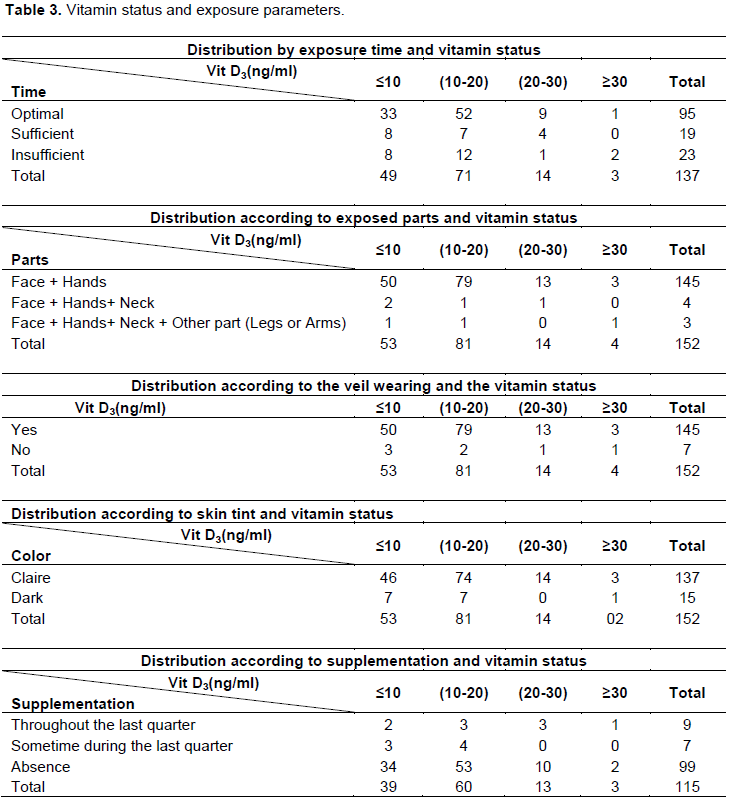
We found 97.37% of hypovitaminosis D of which 9.21% in insufficiency, 88.16% in deficiency (Table 1). Our study population is young, with an average of 29±6 years old. This hypovitaminosis D affects all age groups (Table 1). Statistical analysis shows no correlation between age and vitamin concentration (p = 0.933). Statistical analysis reveals no correlation between BMI and vitamin status (p = 0.536). The phenomenon of severe hypovitaminosis is slightly more severe in period 2 than in period 1. However, the statistical analysis reveals a lack of association between seasonal variation and vitamin status (p = 0.339). The percentage of hyperparathyroidism in the whole sample is 22.37% (Table 2). We note that hypovitaminosis is accompanied by a PTH concentration that increases slightly according to the seasonal distribution: In period 1, the average concentration is the highest in period 2 (Table 2). The correlation statistical study establishes that there is a negative correlation between concentrations of 25 (OH) D3 and that of PTH (p= 0,016). We obtained 60.53% of cases of phosphocalcic balance abnormalities in our sample which are distributed as follows: 4.60% of proven hypocalcemia, 3.29% of hypercalcemia, 7.24% of hyperphosphatemia, 45, 39% hyperactivity of PAL. The phosphocalcic balance is slightly higher in period 1 than in period 2 (Table 2). We were able to collect the sun exposure parameter only from 137 patients (Table 3), and the statistical analysis found no association between the exposure time and the vitamin content of our sample (p = 0.621). Patients wearing the veil and exposing the less extensive skin surface area of ​​exposure of the face and hands represent 95.39%. This group has the highest rate of hypovitaminosis with 88.96% deficiency (Table 3). No association between 25 (OH) D3 and the exposed parts (p = 0.388) nor between 25 (OH) D3 and the haze (p = 0.301) was statistically revealed. 87.59% of the light-skinned population had vitamin D deficiency [25 (OH) D3 <20 ng / ml] compared to 93.33% for dark skin. Statistical analysis reveals a lack of association between skin pigmentation and vitamin concentration in our population (p = 0.220). In period 1, milk is the most consumed food daily (80.88%) in our sample. Next are meat products (38, 24%), butter and margarine (33.82%), eggs (29.41%) and finally fish (5.88%). In period 2, the daily consumption of milk remains the highest (78.26%). This is followed by meat products (56.52%), butter and margarine (33.33%), eggs (30.43%) and fish (0%). The prescribed products were combinations containing vitamin D3 (multivitamin, association with calcium). We were able to collect only 115 data related to this topic. Ninety-nine women were not supplemented, that is, 86.09 and 87% of them had 25 (OH) D3 content <20 ng / ml. Nine women received supplementation throughout the third trimester of pregnancy. 55.55% of them showed vitamin deficiency (Table 3). Statistical analysis indicated a lack of association between supplementation and vitamin D status (p = 0.157). Among the sports activities, the number of patients surveyed is 131. There are 53 female sports practitioners with 90.57% vitamin deficiency. Those who do not practice sport account for 84.61% of vitamin deficiency. There is no association between physical activity and 25 (OH) D3 concentration (p = 0.331).
DISCUSSION
Our study shows that there is a high prevalence of hypovitaminosis D among our sample of Moroccan pregnant women. Fugain and Jacquot (2015) in a similar study of pregnant women in Montpellier found 78% of hypovitaminosis D, of which 30% in insufficiency, 24% in moderate deficiency and 24% in severe deficiency. Studies by Gale et al. (2008), Sachan et al. (2005) and Davis et al. (2010) on samples of 207, 466 and 36 pregnant women respectively showed 42.5, 49.5 and 36.1% vitamin deficiency strict. In Turkey, Pehlivan et al. (2003) reported a 79.5% severe deficiency among 76 women studied. In Iran, Zhila et al. (2007) obtained only 3.4% of optimal status in a population of 552 women. Hypovitaminosis also expose their offspring, which runs a high risk of acquisition of diseases in the short (rickets, growth retardation, hypocalcemic tetanus), average (respiratory or autoimmune diseases) and long-term (early osteoporosis, dementia). 'Alzheimer). Similarly, work has shown in their sampling a vitamin status much better than ours. In the United States, Bodnar et al. (2007) obtained 30.21% deficiency and 35.94% optimal status in a sample of 384 women. In Martinique and the Netherlands, low prevalence of hypovitaminosis was revealed after the study of 63 women by Mbou et al. (2009) (8% deficiency) and 105 indigenous women by Van der Meer et al. (2006) (8% severe deficiency). Negative correlation links vitamin status and PTH content. Our study corroborates this fact established by physiology and by many other studies (Sachan et al., 2005; Zhila et al., 2007). The low occurrence of secondary hyperparathyroidism in our sample characterized by high hypovitaminosis supports the following shade taught by Cormier and Souberbielle (2006). These authors state that vitamin D insufficiency does not inevitably lead to secondary hyperparathyroidism. Only subjects with such concentrations of 25 (OH) D, on average, have higher PTH than those with serum 25 (OH) D above these thresholds, and their PTH decreases when vitamin D is administered. Our study establishes this fact since only 34 of our women (22.37%) presented with hyperparathyroidism, 31 with deficient vitamin content, 2 with insufficient status and 1 with satisfactory status. The statistical study does not reveal periodic fluctuations in vitamin status. The hypovitaminosis of our population is thus ubiquitous regardless of the intensity of sunshine. Lisa McGuire Davis, Van der Meer, and their respective teams also emphasized this trait as a result of their study (Davis et al., 2010; Van der Meer et al., 2006). Our results allow us to affirm that hypovitaminosis D is therefore rife in Morocco even during the summer, even though we are in a sunny country. This paradox has already been raised by national works (Allali et al., 2009) and international (Sachan et al., 2005; Sahu et al., 2009; Grover et al., 2001; Feleke et al., 1999) who have realized the same finding of vitamin deficiency in their country (India, Australia, Ethiopia). Among the first notions of explanation of this phenomenon, the factors preventing endogenous vitamin synthesis are self- evident. The wearing of covering clothes is unanimously recognized as a factor favoring hypovitaminosis D (Sachan et al., 2005; Pehlivan et al., 2003, Allali et al., 2009; Lips et al., 2007; Marie-France et al., 2009; Sonja et al., 2008). Our study similarly supports: the wearing of the veil was adopted by 95.39% of our women who also displayed clothing that left only the face and hands uncovered. This proportion of women alone accounts for 96.27% of women in our sample with 25 (OH) D3 concentrations below 20 ng / ml. Other elements are also responsible for the poor vitamin status of our sample. The body mass index is inversely proportional to the vitamin status. The higher the BMI, the greater the risk of calcidiol deficiency. Our sample includes 62 women (43.36%) whose BMI indicates obesity and 93.55% of them are deficient. 76.19% of women with normal BMI and 88.33% of overweight women are deficient. The relationship between BMI and 25 (OHD) content is purely physiological. Lipophilic vitamin D has a strong affinity for adipocytes which exerts on it a sequestering effect harmful to its bioavailability. The circulating portion is then considerably reduced. As a result, the C25 hydroxyl fraction is also reduced. Other studies (Winters et al., 2008; Bodnar et al., 2007) have established and verified the negative impact of BMI on vitamin status. The food survey in our population revealed that the frequency of consumption of the products richest in vitamin D, namely tuna, sardine, butter, and margarine, is lower in period 2 than in period 1. This finding provides another explanation for the periodic distribution of vitamin content. Milk is proving to be the most consumed food. Unfortunately, this commodity is rarely and poorly supplemented with vitamin D in Morocco. PTH is the hypercalcemic hormone par excellence. Its secretion is modulated in priority by the state of the calcemia. Any elevation of the serum calcium concentration induces inhibition of parathyroid hormone secretion. Similarly, a decrease in serum calcium causes the opposite phenomenon. In our opinion, the high consumption of milk allowed the women in our sample to obtain considerable calcium intake. This made it possible to maintain a normal phosphocalcic balance, despite hypovitaminosis D, thus minimizing the occurrence of secondary hyperparathyroidism. The slight decrease in consumption of dairy products observed in period 2 goes hand in hand with the poorer quality of the phosphocalcic balance evaluated during this period. The protection exerted by the calcemia is relaxed and the hypovitaminosis is more felt, causing an increase in the concentration of PTH. Out of 115 women interviewed, only 16 received supplementation during the last trimester of pregnancy. 81.25% of them were found to be vitamin deficient. This result, as well as the absence of an association between supplementation and 25 (OH) D3 content, both show that the drug supplementation in our sample did not fulfill its palliative role. Supplementation was not uniformly prescribed: some patients received it throughout the trimester and others for some time. A slight tendency to hypovitaminosis is prevalent among women exercising. The link between sports activities and 25 (OH) D3 content was mainly studied in the elderly, where it was found that the practice of exercises increases the risk of falls and fractures which are manifestations of vitamin deficiency (Pierre-Jean et al., 2003). Exercise can thus appear as a predictor of vitamin D status (Giovannucci et al., 2006). The role of vitamin D in muscle metabolism is of considerable importance since it allows, among other things, the maturation of myocytes as well as the oxygenation and calcium supply of striated muscle fibers (Souberbielle et al., 2008; Michèle et al., 2000). Vitamin D deficiency is, therefore, a source of neuromuscular disorders. Our work reveals a similar link in our population of young women. The practice of physical activities requires neuromuscular efforts to the maternal organism which, in response to this demand, draws on the available 25 (OH) D reserve. Vitamin D requirements, like other nutrients in general, increase with gestational age. To avoid vitamin deficiency and all its repercussions, the pregnant woman must take care of her diet and provide sufficient nutritional quantities to her body to ensure adequate vitamin D content.
CONCLUSION
Moroccan women constitute a population at risk, because of their clothing profile (wearing protective clothing). The acquisition of an adequate vitamin D content is the result of a multifactorial optimization, mainly involving sun exposure and dietary intake. Rational use of sunscreens and adequate supplementation seem to us to be necessary and effective control measures. Information campaigns are useful for educating the general public on the benefits of vitamin-sun and the benefits of a vitamin D-rich diet. Prescription vitamin supplements are better for fighting maternal hypovitaminosis and can improve the availability of this substance for the fetus. However, there is currently limited data to directly assess the benefits and harms of vitamin D supplementation alone during pregnancy to improve maternal and infant health. The pregnant woman should be encouraged to receive adequate nutrition, a balanced diet being the best way to achieve this.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Allali F, El Aichaoui S, Khazani H, Benyahia B, Saoud B, El Kabbaj S, Bahiri R, Abouqal R, Hajjaj-Hassouni N (2009). High Prevalence of Hypovitaminosis D in Morocco: Relationship to Lifestyle, Physical Performance, Bone Markers, and Bone Mineral Density. Seminars in Arthritis Rheumatism 38(6):444-51. |
|
|
Bodnar LM, Catov JM, Roberts JM, Simhan HN (2007). Prepregnancy Obesity Predicts Poor Vitamin D Status in Mothers and Their Neonates. The Journal of Nutrition 137(11):2437-2442. |
|
|
Brannon PM, Yetley EA, Bailey RL, Picciano MF (2008). Summary of roundtable discussion on vitamin D research needs. American Journal of Clinical Nutrition 88:587S-592S. |
|
|
Cormier C, Souberbielle JC (2006). Nouvelles définitions de l'insuffisance vitaminique D, retentissement sur les normes de PTH. La Revue de Médecine Interne 27(9):684-689. |
|
|
Daniel ER, Morris SK, Zlotkin S, Gernand AD, Ahmed T, Shanta SS, Papp E, Korsiak J, Shi J, Islam MM, Jahan I (2018). Vitamin D supplementation in pregnancy and lactation and infant growth. New England Journal of Medicine 379(6):535-546. |
|
|
Davis LM, Chang SC, Mancini J, Nathanson MS, Witter FR, O'Brien KO (2010). Vitamin D Insufficiency Is Prevalent among Pregnant African American Adolescents. Journal of Pediatric Adolescent Gynecology 23(1):45-52. |
|
|
Feleke Y, Abdulkadir J, Mshana R, Mekbib TA, Brunvand L, Berg JP, Falch JA (1999). Low levels of serum calcidiol in an African population compared to a North European population. European Journal of Endocrinology 141(4) :358-360.. |
|
|
Fugaina P, Jacquot A (2015). Hypovitaminosis D pendant la grossesse: Prévalence et facteurs de risque. Étude prospective observationnelle au CHRU de Montpellier. La Revue Sage-Femme 14(3):85-93. |
|
|
Gale CR, Robinson SM, Harvey NC, Javaid MK, Jiang B, Martyn CN, Godfrey KM, Cooper C; Princess Anne Hospital Study Group (2008). Maternal vitamin D status during pregnancy and child outcomes. European Journal of Clinical Nutrition 62(1):68-77. |
|
|
Giovannucci E, Liu Y, Rimm EB, Hollis BW, Fuchs CS, Stampfer MJ, Willett WC (2006). Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. Journal of National Cancer Institute 98(7):451-459. |
|
|
Grover SR1, Morley R (2001). Vitamin D deficiency in veiled or dark-skinned pregnant women. The Medical Journal of Australia 175(5):251-252. |
|
|
IOM (Institute of Medicine) (2011). Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: The National Academies Press. |
|
|
Jing Yuan, Pu Jia, Lin Hua, Zhong Xin and Jin-Kui Yang (2019). Vitamin D deficiency is associated with risk of developing peripheral arterial disease in type 2 diabetic patients. BMC Cardiovascular Disorders 19(1):145. |
|
|
Lips P (2007). Vitamin D status and nutrition in Europe and Asia. Journal of Steroid Biochemistry & Molecular Biology 103(3-5):620-625. |
|
|
Marie-France LG, Christian D, Ambroise M, Nicolas M, Pascal Q, Anne-Marie S, Martine L, Contardo G (2009). L'hypovitaminose D chez les femmes jeunes : une réalité sous-estimée. Cahiers de nutrition et de diététique 44(6):264-272. |
|
|
Mbou FM, Pagès-Lutzb F, Garabédian M, Walrant- Debray O, Leguyader P, Robert P, Pierrisnard E (2009). Statut vitaminique D maternel à la Martinique : Étude prospective de décembre 2004 à avril 2005 sur 63 femmes enceintes à terme. Journal de Gynécologie Obstétrique et Biologie de la Reproduction 38(2):161-167. |
|
|
Michèle Garabedian (2000). La 1,25- dihydroxyvitamine D et son recepteur. Revue du Rhumatisme 67(2):39-41. |
|
|
Mulligan ML, Felton SK, Riek AE, Bernal-Mizrachi C (2010). Implications of vitamin D deficiency in pregnancy and lactation. American Journal of Obstetrics and Gynecology 202(5):429-e1. |
|
|
Omeed S, Swapnil K, Amy G (2020). Vitamin D Deficiency. Treasure Island (FL): StatPearls Publishing. |
|
|
Pehlivan I, Hatun S, AydoÄŸan M, BabaoÄŸlu K, Gökalp AS (2003). Maternal vitamin D deficiency and vitamin D supplementation in healthy infants. The Turkish Journal of Pediatrics 45(4):315-320. |
|
|
Pierre-Jean M, Pawel S (2003). Synergie des effets de la vitamine D et du calcium dans la prévention de la fracture de l'extrémité supérieure du fémur chez les sujets âgés. Revue du Rhumatisme 5(70):359-362. |
|
|
Sahu M, Bhatia V, Aggarwal A, Rawat V, Saxena P, Pandey A, Das V (2009). Vitamin D deficiency in rural girls and pregnant women despite abundant sunshine in northern India. Clinical Endocrinology 70(5):680-684. |
|
|
Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V (2005). High prevalence of vitamin D deficiency among pregnant women and their newborns in northern India. American Journal of Clinical Nutrition 81(5):1060-1064. |
|
|
Sophie C, Jean-Philippe K, Aline R, Magdeldin E, Alexandra N, Sabine R, Katharina C, Quack L (2019). Vitamin D status and its determinants in healthy pregnant women living in Switzerland in the first trimester of pregnancy. BMC Pregnancy Childbirth 19(1):10. |
|
|
Souberbielle JC, Prié D, Courbebaisse M, Friedlander G, Houillier P, Maruani G, Cavalier E, Cormier C (2008). Actualité sur les effets de la vitamine D et l'évaluation du statut vitaminique D. Annales d'Endocrinologie 69:501-510. |
|
|
Sonja B, Ambroise M, Anne-Marie S, Martine L, Marie-France LG (2008). La carence en vitamine D chez la femme de 18 à 49 ans portant des vêtements couvrants, une réalité méconnue en médicine générale. Presse Médicale 37:201-206. |
|
|
Stefan P, Armin Z, Christian T, Verena TS, Elisabeth L, Martin HK, Martin RG, Winfried M, Marlene P (2019). Vitamin D testing and treatment: a narrative review of current evidence. Endocrine Connections 8(2):27-43. |
|
|
Van der Meer IM, Karamali NS, Boeke AJ, Lips P, Middelkoop BJ, Verhoeven I, Wuister JD (2006). High prevalence of vitamin D deficiency in pregnant non-Western women in The Hague, Netherlands. American Journal of Clinical Nutrition 84(2):350-353. |
|
|
Zhila M, Arash HN, Ali RS, Farzaneh K, Farzaneh SM, Bagher L (2007). Vitamin D status in mothers and their newborns in Iran. BioMed Central Pregnancy and Childbirth 7:1. |
|
|
Wagner CL, Hollis BW, Kotsa K, Fakhoury H, Karras SN (2017). Vitamin D administration during pregnancy as prevention for pregnancy, neonatal and postnatal complications. Reviews in Endocrine and Metabolic Disorders 18(3):307-322. |
|
|
Winters SJ, Chennubhatla R, Wang C, Miller JJ (2009). Influence of obesity on vitamin D-binding protein and 25-hydroxy vitamin D 138 levels in African American and white women. Metabolism Clinical and Experimental 58(4):438-442. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


