Full Length Research Paper
ABSTRACT
Type 2 diabetes mellitus (T2DM) is characterized by chronic hyperglycemia and associated with an increased production of reactive oxygen species (ROS) affecting beta cells in pancreas. Glutathione S- transferases (GSTs) are a family of antioxidant enzymes that include several classes of GSTs. These enzymes have important roles in decreasing ROS species and act as a kind of antioxidant defense. In a case-control study, the role of GSTMI and TI polymorphisms in predisposition for T2DM using multiplex polymerase chain reaction in 103 T2DM patients and 170 healthy controls from Turabah Province, Saudi Arabia was investigated. GSTM1 null variant was associated with higher genetic risk predisposing to T2DM in the study population. Our study revealed that individuals who are GSTM1 null genotype are associated with 1.863 times risk for predisposition to T2DM (Odds ratio = 1.863; 95% CI = 1.265 - 2.742; P-value=0.00001). While GSTT1 polymorphism has no role in genetic predisposing to T2DM in the study population (Odds ratio = 1.053; 95% CI = 0.921 - 1.203) and its contribution in susceptibility for T2DM was only detected with combined double deletions with GSTM1 null variant in the population (P-value = 0.041, Odds Ratio = 1.104; 95% CI = 0.991 - 1.230). These results indicated that individuals who have GSTM1 null variant or GSTM1 and GSTT1 double deletion are at higher risk for developing T2DM than those who are positive genotyped for GSTT1gene.
Key words: T2DM, glutathione S-transferase, Genetic polymorphisms, Turabah, SA.
INTRODUCTION
Diabetes Mellitus (DM) is one of the most common chronic diseases in the world. The disease is characterized by metabolic abnormalities and long-term complications involving the eyes, kidneys, nerves, and blood vessels (Powers, 2005). The number of people with DM worldwide was estimated to exceed 336 million in 2011 and most of them have type 2 diabetes mellitus (T2DM). The highest regional prevalence during 2011 was in Middle East and North Africa. In the Middle East region, Saudi Arabia and Iran had the greatest diabetic prevalence among other regional countries (Whiting et al., 2011).
T2DM is a multifactorial heterogeneous group of disorders characterized by a deficiency or failure in maintaining normal glucose homeostasis resulting from defects in insulin secretion and insulin action (Marchetti et al., 2009). The disease accounts for the majority of all diagnosed cases of diabetes in adults that is typically associated with obesity, sedentary lifestyle, older age, family history of diabetes, and ethnicity (Bayness and Thorpe, 1999; Zimmet and Shaw, 2001). T2DM is a risk factor for microvascular complications leading to limb amputations, renal failure, and blindness, as well as other disorders such as hypertension, cardiovascular disease, dyslipidemia, and infections. T2DM is associated with an increased production of reactive oxygen species (ROS) together with reduction of antioxidant defenses. This leads to accumulation of free radicals in tissues (oxidative stress) which specially affects beta cells in pancreas and may play an important role in the development of diabetes and its complications (Giron and Saito, 1999). Several studies have demonstrated that individuals with lowered antioxidant capacity are at increased risk of T2DM (Bayness and Thorpe, 1999; Gallou et al., 1993).
The glutathione-S-transferases (GST) are key phase II enzymes and they play critical roles in protection against products of oxidative stress and electrophiles. They are involved in the conjugation of a wide range of electrophilic substances with glutathione, thus facilitating detoxi?cation and further metabolization and excretion. At least ?ve related gene families, mu, alpha, pi, theta and sigma have been identi?ed in humans. Genetic polymorphisms have been reported for GSTM1, GSTP1 and GSTT1, resulting in either decreased or altered enzyme activity. Five mu class genes (M1–M5) have been identi?ed on chromosome 1p13 (Whalen and Boyer, 1998).
Several investigations have determined the clinical or genetic factors associated with T2DM with interest to detoxification agents. Study from China has demonstrated a significant association of the null mutation of GSTTI gene and T2DM, but in Turkish and North Indian researches, this association was observed between GSTM1 deletion and T2DM. Moreover, North Indian study was the only research that reported significant association of the point mutation of GSTP1 gene and T2DM (Bid et al., 2010; Wang and Li, 2006).
In this case-control study we investigated the association of the GSTs polymorphisms with type 2 diabetes mellitus among population of Turabah province. No similar studies had been done in Kingdom of Saudi Arabia (KSA). Knowing the genetic factors in predisposition to type 2 diabetes mellitus in Saudi population will help in identifying individuals at higher risk of developing the disease and help in regular follow up for preventive measures to decrease the morbidity and mortality among type 2 diabetic patients.
MATERIALS AND METHODS
Study area and population
A case-control study was conducted at Turabah General Hospital in Turabah province (western region, KSA) to investigate the role of GST polymorphisms in the genetic predisposition to type 2 diabetes mellitus among population of Turabah province. A sample of 103 T2DM diabetic patients was randomly selected from known T2DM patients who visit the General Hospital of Turabah or Medical Health Centers for routine follow up. For the purpose of our case- control study, blood samples were collected from randomly selected 170 unrelated healthy persons (who never have a history of Diabetes mellitus, matching in age, older, and sex) from the Turabah population. Informed consent was obtained from all participants at the time of blood withdrawal and collection of patients` clinical and pathological data. Patients who refuse to participate in the study or to donate blood, who had life-threatening disease or whose clinical and pathological data are not available were excluded from the study.
Study subjects
Blood samples were collected from the healthy control individuals and T2DM patients, who were born and are living in Turabah Province, after their acceptance to participate in the study. The mean age of the study subjects was 44.87 ± 10.46 years old; the minimum age is 30 years old and the maximum is 60 years old. 98 (60%) are males and 66 (40%) are females. The study was approved by the Ministry of Health and Research Committee at Taif University.
Genomic DNA extraction
Genomic DNA was extracted from peripheral blood using standard procedures [12]. Briefly, 5 ml of blood was mixed with an equal volume of RBC lysis buffer (0.32M sucrose, 5mM MgCl2, 10% triton X-100, and 12mM Tris–HCl, pH 8.0) and allowed to sit for 5 min. The cell lysate was then centrifuged at 2000 rpm and the upper layer was discarded. The pellets were re-suspended in phosphate buffered saline (PBS; pH 7.4) and 1% sodium dodecyl sulfate, and then digested with 0.2 mg/ml proteinase K at 55°C overnight. After digestion, the DNA was purified using phenol-chloroform extraction, followed by ethanol precipitation with 0.3M potassium acetate (pH 5.2). The DNA was finally stored in TE (10mM Tris–HCl and 1Mm EDTA, pH 8.0) until use.
Genotyping of GSTM1 and GSTT1 polymorphisms in subjects and control groups
GSTM1 and GSTT1 genotypes were identified by using a multiplex PCR-based method and three sets of primers
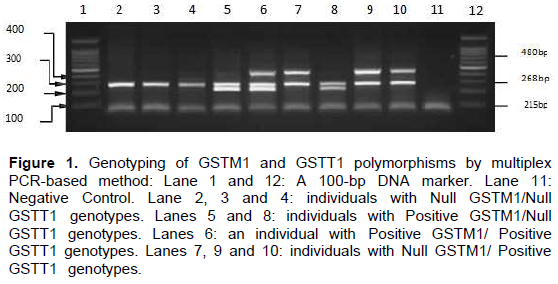
The sequences for the GSTM1 forward and reverse primers were; 5`-gAACTCCCTgAAAAgCTAAAgC-3`and 5`- gTTgggCTCAAATATACggTgg-3` (Bell, 1993) Sequences for the GSTT1 forward and reverse primers are 5`- TTCCTTACTggTCCTCACATCTC-3` and 5`- TCACCggATCATgg CCAgCA-3`[15] To be certain that a null genotype is due to the absence of GSTM and GSTT1 alleles rather than a failure in the PCR analysis, we had co-amplified human β- globin using primers 5`-CAACTTCATCCACgTTCACC-3` and 5`- gAAgAgCCAAggACAggTAC-3` as internal control. The PCR reaction was carried out in an Applied Biosystem 9700 Thermocycler in a total of 25 μl reaction mixture containing: 50-100 ng of genomic DNA; 1.6 mM dNTPs; 200 nM of each GSTM1, GSTT1, and β-globin primer (Cinnagen, Iran); 10mM Tris_/HCI (pH 9.2); 50 mM KCl; 2 mM MgCl2; and 1.5 units of Taq polymerase. Cycling conditions were an initial denaturation for 4 min at 93°C, followed by 45 s at 61°C and 90 s at 72°C for one cycle, followed by additional 36 cycles of 93°C for 30 s, 63°C for 45 s, and 72°C for 90s. The PCR products were resolved on an ethidium bromide-stained 1.7% 1:1 NuSieve/MP agarose gel together with a DNA molecular weight marker. Amplification with β-globin primers produces a 268 base pair band indicating that the PCR reaction is reliable.
The presence of a 215 base pair band indicates that this subject is primers for GSTM1 homozygote or heterozygote while its absence in the presence of the internal control band indicates the Null GSTM1. The presence of a 480 base pair band indicates that this subject is homozygote or heterozygote for GSTT1 while its absence in the presence of the internal control band indicates the Null GSTT1.
Statistical analysis
The allele/genotype frequencies of the different genes polymorphism were determined and had been tested for Hardy- Weinberg equilibrium for both patient and control groups using the χ2 test. The same test will be used to evaluate significant associations between the diseases (T2DM versus controls). The differences between different groups were considered significant if the P-value is not exceeding 0.05. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by unconditional logistic regression. When expected values in contingency tables are under 5, Fisher's exact test was used to analyze the data. For GSTM1 and GSTT1 present genotypes, we calculated the genotypes frequencies of heterozygous and homozygous present in both T2DM and healthy control groups predicated from GSTM1 null genotype frequencies in each group according to Hardy-Weinberg Equilibrium (HWE);
p2 + 2pq + q2 = 1
Assuming GSTM1 null genotype frequency as (p2), we calculated the allele frequencies and genotypes frequencies of heterozygous and homozygous present in both groups.
RESULTS
Figure 1 shows the genotype frequencies of GSTM1 and GSTT1 polymorphisms among the T2DM patients and their healthy controls groups. 76 (76%) of T2DM patients were GSTM1 null while 24 (24%) were GSTT1 null genotypes. The double deletions of both GSTM1 and GSTT1 null were detected in only 19 (19%) of T2DM. Among healthy control group, GSTM1 null genotypes were only detected in 94 (55%) and GSTT 1 null genotypes were detected in 34(20%) while 18(10%) of healthy control were double deletions for both GSTM1 and GSTT1 null genotypes.
The association of GSTM1 polymorphism and T2DM in study population
Calculation of GSTM1 genotypes and allele frequencies in T2DM and healthy control groups
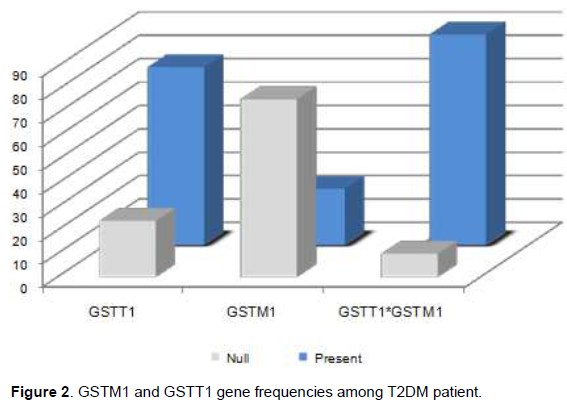
The estimated different genotypes and gene frequencies predicated from GSTM1 null genotype frequencies in T2DM and healthy control groups according to Hardy- Weinberg Equilibrium (HWE) (Figure 2). GSTM1 null genotype frequency (p2) in T2DM group was 0.76 and in healthy control group was 0.55. Thus, the estimated GSTM1 null allele frequency was 0.87 in T2DM patients and 0.74 in healthy control. The calculated GSTM1 present allele frequencies (q) in T2DM group and in healthy control groups were 0.13 and 0.26; the heterozygote and homozygous present frequencies were 0.22 and 0.02 in T2DM group while in healthy were 0.38 and 0.07 respectively. There was significant increase in GSTM1 null allele frequency in T2DM patients group than that in healthy control group (P-value = 0.0001) (Table 1). The distribution of GSTM1 polymorphism genotypes in healthy control group was consistent with the Hardy- Weinberg equilibrium but significantly different in comparison with its genotypes distribution among T2DM patient group (P-value= 0.005).

GSTM1 Null variant is strong genetic risk factor for development of T2DM among study population
The distribution of GSTM1 polymorphism null and present genotype in T2DM patients and healthy controls groups is shown in Table 2. There was significant increase in GSTM1 null genotype frequency in T2DM patients group than that in healthy control group (P-value = 0.0001). This indicated that individuals who are Homozygous for GSTM1 null gene had 1.86 times increased risk for developing of T2DM than those who have GSTM1 present either homozygous or heterozygous (Odds ratio = 1.863 ; 95% CI = 1.265 – 2.742).
Calculation of GSTT1 genotypes and allele frequencies in T2DM and healthy control groups
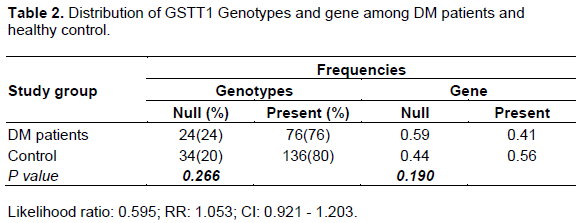
The estimated different genotypes and gene frequencies predicated from GSTT1 null genotype frequencies in T2DM and healthy control groups according to Hardy- Weinberg Equilibrium (WBE) are shown in Figure 3 and Table 2. GSTT1 null genotype frequency (p2) in T2DM group was 0.24 and in healthy control group was 0.20. Thus, the estimated GSTT1 null allele frequency was 0.59 in T2DM patients and 0.45 in healthy control. The calculated GSTT1 present allele frequencies (q) in T2DM group and in healthy control groups were 0.41 and 0.55 while the heterozygote and homozygous present genotype frequencies were 0.50 and 0.26; in healthy group, it was 0.49 and 0.31 respectively. There was no significant difference in GSTT1 null allele frequencies in T2DM and healthy control groups (P-value = 0.266). The distribution of GSTT1 polymorphism genotypes in T2DM and healthy control groups was consistent with the Hardy-Weinberg equilibrium (P-value= 0.666).
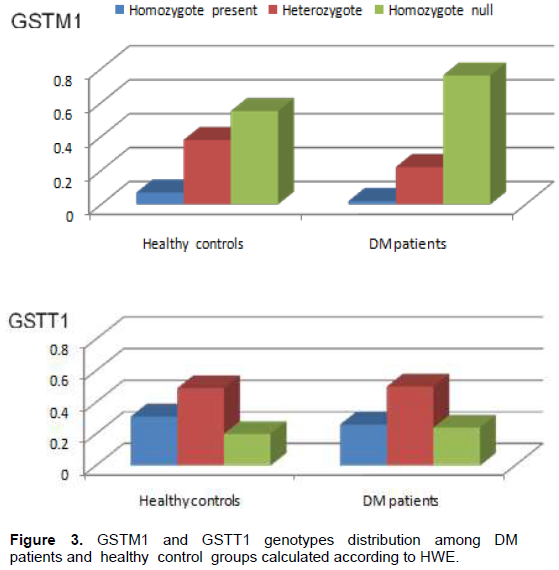
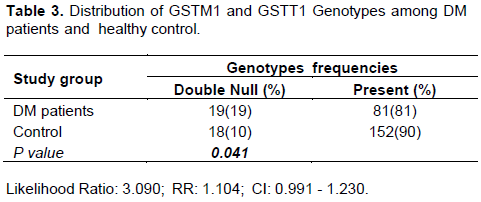
The double deletions of both GSTM1 and GSTT1 were detected in 19% of T2DM and only in 10% of healthy control (Table 3). This observation indicates that individuals who are GSTM1 and GSTT1 genes double deletion are at higher risk for developing T2DM than those who are positive genotyped for both or either GSTM1 and GSTT1 genes (RR: 1.104; CI: 0.991 – 1.230, P-value = 0.041).
DISCUSSION
In pancreatic β-cells, the presence of low levels of antioxidants makes them highly sensitive to cytotoxic stresses associated with higher risk for oxidative damage; it is also associated with an increased production of reactive oxygen species (ROS) together with reduction of antioxidant defenses (Robertson et al., 2003). This leads to the accumulation of free radicals in tissues (oxidative stress) which specially affects β-cells in pancreas. This plays an important role in β-cells damage and subsequently in the development of diabetes and its complications (Giron and Saito, 1999). Several studies have demonstrated that individuals with lowered antioxidant capacity are at increased risk of T2DM (Bayness and Thorpe, 1999; Gallou et al., 1993).
Family of GSTs enzymes is a major component of phase II xenobiotics, drugs metabolizing and antioxidant system (Wang et al., 2006). GSTM1 is a separate isoform of glutathione transferase enzymes that participates in the metabolism of a wide range of chemicals. Known substrates for the GSTM1 enzyme include reactive peroxide intermediates generated from the activation of polycyclic aromatic hydrocarbons by cytochrome P450 enzymes (Hayes and Pulford, 1995). Polymorphisms reducing or eliminating these enzyme detoxification activities could be associated with increased genetic susceptibility to complex human diseases including T2DM (Hayes, and Pulford, 1995; Yalin, 2007). Deletion variants that are associated with a lack of enzyme function exist at both these loci. Individuals who are carriers of homozygous deletions in the GSTM1 gene may have an impaired enzyme activity. Although, frequencies of homozygousGSTM1 deletion carriers is very high (30-50%) in most populations studied to date (London, 1995).
Our study revealed that GSTM1 null genotype was associated with 1.86 times increased risk for developing of T2DM than those who are GSTM1 present either homozygous or heterozygous increased risk for predisposition to T2DM in the study population. Several previous studies done in other populations are consistent with our observation in the study population (Yi et al., 2013). Significant associations of GSTM1 null genotype with development of T2DM were reported in populations of Southern and Northern parts of India (Bid et al., 2010; Ramprasath, 2011; Raza, 2014). Strong association of the GSTM1 null genotype and predisposition to T2DM was observed in Turkish population (Yalin, 2007). Nevertheless, a study from Iran indicated that GSTM1 null variant was significantly increased in T2DM patients and might be involved in the pathogenesis of T2DM in South Iranian population (Moasser, 2012). However, inconsistency was observed in some other populations, where no association between GSTM1-null and T2DM was observed in the Brazilian population (Pinheiro, 2013). While, genetic susceptibility to diabetes mellitus in Chinese population was reported not to be affected by GSTM1 polymorphism (Wang et al., 2006). Furthermore, no association was detected in Egyptian diabetic patients (Moyassar et al., 2015).
Our results suggest that the absence or reduced activity of detoxification pathway of GSTM1 has significant effect on genetic risk predisposing to T2DM in Saudi population in Turabah province, Western region. The reduced anti-oxidant capacity among diabetic patients with GSTM1 null genotypes together with other known genetic risk markers could have some important implications in identifying individuals with higher predisposition for disease that may facilitate possible interventions in prevention or delaying onset of the disease, proper diagnosis and management, in order to improve disease`s prognosis.
Lack of association of GSTT1 polymorphism and susceptibility to T2DM in study population
Several previous studies had documented that GSTT1 present genotype could confer protection against the development of T2DM (Wang et al., 2006; Amer, 2011; Hori, 2007). In this study, GSTT1 polymorphism different genotypes were evaluated for their association with susceptibility to T2DM. There were no significant differences both in the genotypes distributions and in the alleles frequencies of the GSTT1 polymorphism for the patients and the control group. This indicated that GSTT1 polymorphism has no role in genetic risk predisposing to T2DM in study population. Same observation was verified by several studies conducted in other population and documented no association between GSTT1 polymorphisms and T2DM (Hori, 2007; Datta, 2010). In addition, an Indian population study reported no significant association of GSTT1 polymorphism with T2DM (Bid et al., 2010). On the other hand, inconsistencies to our observation were reported in few studies in other populations. In Brazilian population, was suggested that the GSTT1 polymorphism could play an important role in the pathogenesis of T2DM (Pinheiro, 2013) while, a double fold higher risk of GSTT1 null genotype for predisposition to T2DM was reported in Iraqi population (Al-Mayah, 2014).
Despite some inconsistency in the literature data, GSTT1-null and GSTT1-null/GSTM1-null genotypes have consistently been considered risk factors for the development of T2DM as reported by a meta-analysis study (Bid et al., 2010). In addition, there several studies reported significant association to T2DM for both null genotypes of GST [24, 29]. Others verified that there was no association between GSTT1 and GSTM1 polymorphisms and T2DM (Hori, 2007; Datta, 2010). In addition, others studies showed that only the GSTM1-null genotype may play a significant role in the pathogenesis of T2DM (Bid et al., 2010). The contribution of GSTT1 null genotype in susceptibility for T2DM in this study was only detected when it was combined with GSTM1 null variant in this population. Since GSTT1 null genotype has no role in T2DM susceptibility in this study, we can suggest that the significant association of GSTM1/GSTT1 double deletions in this study population could be mainly due to the combined GSTM1 deletion. This was supported by that reported in other studies and indicated that only the GSTM1-null genotype could play a significant role in the pathogenesis of T2DM (Bid et al., 2010).
CONCLUSION
GSTM1 null variant was associated with two-fold risk for predisposition to T2DM. The absence or reduced activity of detoxification pathway of GSTM1 that results from deletion has a significant effect on genetic risk predisposing to T2DM in Saudi population from Turabah province, Western region. In this study, although GSTT1 polymorphism has no role in genetic risk predisposing to T2DM, its contribution in susceptibility for T2DM was only detected when combined in double deletions with GSTM1 null variant.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors thank all the participants for participating in this study and the clinicians and laboratory staff at Turabah General Hospital for their support in the selection of study participants. This study is a part of the Genetic of Metabolic Diseases research project that was funded by Research Center, Taif University, Saudi Arabia.
REFERENCES
|
Al-Mayah AIA (2014). Association between GSTT1 and GSTM1 genes polymorphisms Type II diabetes miletus patients in Basra Iraq International. Journal Current Microbiology Applied Science 3(11):288-299. |
|
|
Amer MA (2011). Influence of glutathione S-transferase polymorphisms on type-2 diabetes mellitus risk. Genetics and Molecular Research 10(4):3722-3730. |
|
|
Bayness JW, Thorpe SR (1999). Role of oxidative stress in diabetic complications: a new perspective to an old paradigm. Diabetes 48(1):1-9. |
|
|
Bell DA (1993). Genetic risk and carcinogen exposure: a common inherited defect of the carcinogen-metabolism gene glutathione Stransferase M1 (GSTM1) that increases susceptibility to bladder cancer. Journal of the National Cancer Institute 85(14):1159-1164. |
|
|
Bid HK, Hayes KR, Saxena M (2010). Association of glutathione S- transferase (GSTMI, TI and PI) gene polymorphisms with type 2 diabetes mellitus in north Indian population. Journal of Postgraduate Medicine 3(56):176-181. |
|
|
Datta SK (2010). Association of glutathione S-transferase M1 and T1 gene polymorphism with oxidative stress in diabetic and nondiabetic chronic kidney disease. Ren Fail 32(10):1189-1195. |
|
|
Gallou G, Ruelland A, Legras B, Maugendre D, Allannic H, Cloarec L (1993). Plasma malondialdehyde in type 1 and type 2, diabetic patients. Clinica chimica acta 214(2):227-234. |
|
|
Giron MD, Saito RGY (1999). Modulation of hepatic and intestinal glutathione S-trdnsferases and other antioxidant enzymes by dietary lipids in streptozotocin diabetic rats. Chemosphere 38(13):3003-3013. |
|
|
Hayes JD, Pulford DJ (1995). The glutathione S-transferase supergene family: regulation of GST and the contribution of the isoenzymes to cancer chemoprotection and drug resistance. Critical Reviews in Biochemistry and Molecular Biology 30(6):445-600. |
|
|
Hori M (2007). Combined glutathione S-transferase T1 and M1 positive genotypes afford protection against type 2 diabetes in Japanese. Pharmacogenomics 8(10):1307-1314. |
|
|
London SJ (1995). Polymorphism of glutathione S-transferase M1 and lung cancer risk among African-Americans and Caucasians in Los Angeles County, California. Journal of the National Cancer Institute 87(16):1246-1253. |
|
|
Marchetti PLR, Del Guerra S, Bugliani M, D'Aleo V, Occhipinti M, Boggi U, Marselli L, Masini M (2009). Goals of treatment for type 2 diabetes: beta-cell preservation for glycemic control. Diabetics Care 32(2):178-183. |
|
|
Moasser E (2012). Study of the association between glutathione S- transferase (GSTM1, GSTT1, GSTP1) polymorphisms with type II diabetes mellitus in southern of Iran. Molecular Biology Reports 39(12):10187-10192. |
|
|
Moyassar AZ, Thanaa FM, Mona MKEl-D, Amira HM, Noha AAM (2015). Glutathione S-transferase M1, T1 and P1 gene polymorphisms and the risk of developing type 2 diabetes mellitus in Egyptian diabetic patients with and without diabetic vascular complications. Alexandria Journal of Medicine 51(1):73-82. |
|
|
Pinheiro DS (2013). Evaluation of glutathione S-transferase GSTM1 and GSTT1 deletion polymorphisms on type-2 diabetes mellitus risk. PLoS One 8(10):e76262. |
|
|
Powers AC (2005) Diabetes Mellitus. In: Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser SL Jameson JL, Eds, Harrison's Principles of Internal Medicine, 16th Edition, McGraw-Hill, New York pp. 2152-2180. |
|
|
Ramprasath T (2011). Potential risk modifications of GSTT1, GSTM1 and GSTP1 (glutathione-S-transferases) variants and their association to CAD in patients with type-2 diabetes. Biochem Biophys Res Commun, 407(1):49-53. |
|
|
Raza S (2014). Association of Glutathione-S-Transferase (GSTM1 and GSTT1) and FTO Gene Polymorphisms with Type 2 Diabetes Mellitus Cases in Northern India. Balkan Journal of Medical Genetics 17(1):47-54. |
|
|
Robertson RP, Harmon J, Tran PO, Tanaka Y, Takahashi H (2003). Glucose toxicity in beta-cells: Type 2 diabetes, good radicals gone bad, and the glutathione connection. Diabetes 52(3):581-587. |
|
|
Wang G, Li Q (2006). Genetic polyrnorphisms of GSTII, GSTM1, and NQol genes and diabetes mellitus risk in Chinese population. Biochemical and Biophysical Research Communications 341(2):310-313. |
|
|
Wang G, Zhang L, Li Q (2006). Genetic polymorphisms of GSTT1, GSTM1, and NQO1 genes and diabetes mellitus risk in Chinese population. Biochemical and Biophysical Research Communications 341(2):310-313. |
|
|
Whalen R, Boyer TD (1998). Human glutathione S-transferases. Seminars in Liver Disease 18(4):345-358. |
|
|
Whiting DR, Guariguata L, Weil C, Shaw J (2011). IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes research and clinical practice 94(3):311-321. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


