Full Length Research Paper

ABSTRACT
Advanced midwives are expected to be candidates for middle managers in the next generation. Higher levels of management skills than the current levels may be required for middle managers in the future due to the progress of perinatal medicine. The aim of this study was to compare levels of management skills that are currently required for middle managers and levels of management skills that will be important in the next 10-20 years in advanced midwives. A self-administered questionnaire survey was conducted for 1652 advanced midwives in hospitals that have more than 300 beds in Japan. The scores for all management skills that will be required in the next generation were significantly higher than those for currently required management skills. Currently required management skills that were given high scores, including communication ability, ability to perform safety management and problem-solving ability, were also given high scores for middle managers in the next generation. Advanced midwives believed that management skills including the ability to participate in social activity, ability to use information and communication technology, and ability to participate in management in which these scores are low at present are needed for middle managers in the next generation. Advanced midwives consider that management skills for middle managers will change in the future. By acquisition of high levels of management skills, middle managers will be able to perform management of perinatal medicine and nursing.
Key words: Advanced midwives, nursing middle managers, next generation, management skills.
INTRODUCTION
Various current social situations in Japan such as late marriage, late birth, low birth rate and isolation of child-rearing are affecting perinatal medical care. We previously reported that many advanced midwives expected that there would be changes in perinatal care and nursing in the next 10 to 20 years in Japan (Abe et al., 2020). Due to the declining birth rate in Japan, maternity wards have been incorporated into other departments of hospitals and there are concerns about the safety of the maternity environment. In mixed wards, issues regarding the risk of infections in neonatal infants (Kitajima, 2008) and inability for midwives to provide professional midwifery care (Teraoka et al., 2019) have been raised. Postpartum depression is one of the most common complications in the postpartum period, and there have been many studies on risk factors and management for postpartum depression (Guille et al., 2013; Hutchens and Learney, 2020). In Japan, it has been pointed out that support for mental health is necessary to prevent suicide in postpartum women with depression (Asano et al., 2018). Support including medical checks for women at 2 weeks postpartum has therefore been started in Japan, and a system for postpartum care has been established (Ministry of Health, Labour and Welfare, 2019). It is expected that midwives can use their experience to provide effective midwifery care in order to support child-bearing women and postpartum women. However, there has been no indicator for objective assessment of the ability of midwifery practice after obtaining a license to practice midwifery in Japan. The Japan Institute of Midwifery Evaluation developed the Clinical Ladder of Competencies for Midwifery Practice (CLoCMip?) and started a certification system in 2015 for advanced midwives who have acquired level III of the clinical ladder and can provide midwifery care independently (Japan Nursing Association, 2016). Thus, a midwife who can play an active role with a high ability of midwifery practice after acquisition of certification was defined as an advanced midwife in Japan. This definition may be different from the concept of advanced midwifery practice in other countries (Goemaes et al., 2016). Approximately 12,000 midwives are now certified as advanced midwives in Japan. Advanced midwives are expected to be candidates for middle managers in the next generation since they have learned management skills through their experiences of midwifery practice. Middle managers who have important roles in maternity hospitals are required to have diverse management abilities such as the ability to train midwives for improving the quality of midwifery care, the ability to establish a system in which postpartum women can continuously receive midwifery care after leaving a maternity hospital, and the ability to participate in hospital management (Ohira, 2007). The Japan Institute of Midwifery Evaluation indicated items such as safety, economy and leadership as management skills that are required for advanced midwives (Japan Nursing Association, 2013). A higher level of management skills may be required in the future due to the progress of perinatal medicine.
It has been reported that management skills such as ability for adjustment of interpersonal relationships, ability to set goals, ability to show leadership, ability of organization change and ability to conceptualize are required for middle managers in nurses but that it is difficult to obtain these abilities only by training (Ibe et al., 2012). Also, with respect to training middle nursing managers, training of leaders in the next generation is an important issue and the establishment of an evaluation method for education of leaders is needed (Harada, 2014). Thus, management skills that are required for middle managers and programs for training of managers in the next generation in nurses have been established in previous studies. However, management skills that will be required for middle managers in the next generation in advanced midwives have not been clarified.
The aim of this study was to compare the levels of management skills that are currently required for middle managers with the levels of management skills that will be required in the next 10-20 years and to determine the differences in management skills that advanced midwives consider will be required for middle managers in the next generation. A middle manager in the next generation in perinatal care was defined a midwife who had experience of management in a perinatal medical center for 10-20 years and who was playing the role of head nurse as the person in charge of providing nursing services based on the definition of a head nurse by Moriyama and Hunashima (2015). Management skill has been defined as effective action in situations that require management (Katz, 1974).
MATERIALS AND METHODS
This study was conducted during the period from November 2018 to May 2019 in Japan. The subjects for this study were certified advanced midwives, and midwives who did not perform midwifery were excluded. Through a website of the Japan Institute of Midwifery Evaluation, 267 university hospitals, general hospitals and specialized hospitals for mothers and children that have 300 or more beds were selected out of the hospitals in which advanced midwives who were certified in 2015 and 2016 have been working. There were about 3000 certified advanced midwives working in 267 hospitals. The necessary sample size was calculated to be 550?by using permissible errors (5%), reliability (99%) and response ratio (50%), and the appropriate sample size was determined to be 1100 considering the recovery rate (50%). Furthermore, we determined the appropriate sample size to be 1650 considering the recovery rate by mail (20-30%). We sent request forms that stated the aim, significance and methods of the study, and questionnaire forms to chiefs of nursing managers of those hospitals. An acceptance or disapproval for research cooperation was required. For 1652 advanced midwives working in 193 hospitals from which acceptance for research cooperation was obtained, we sent an explanation sheet for the study, an informed consent form, a self-administered questionnaire form and a return envelope. The respondents were requested to send back their completed questionnaire forms. After the acceptance of chief managers of nursing in 193 (72.3%) of the 267 hospitals, 1206 questionnaire forms from 1652 advanced midwives in the 193 hospitals were received (response rate: 73.0%). Sixty-six questionnaires for which there was no check in a check box or there were incomplete answers were excluded, and 1140 questionnaires were used for analysis (effective response rate: 94.5%).
The questionnaire used in this study was a self-developed form. Based on management skills for middle nursing managers that were shown in previous studies in Japan (Motomura and Kawaguchi, 2013; Inoue, 2014; Suzuki and Suzuki, 2018), 22 items of management skills were selected for validity and reliability. A pilot study was conducted for 10 advanced midwives who worked in a hospital with more than 600 beds in order to ensure validity and reliability. Consistency between management skills and contents in the 22 items, easiness for answering, easiness for understanding and a feeling of burden for answering were evaluated. After confirmation of high evaluation of the contents of all items, it was decided to use the questionnaire.
The first part of the questionnaire was questions on basic characteristics including questions on age, years of midwifery experience, position, years of experience in middle management, training institution for obtaining a midwife license, type of affiliated facility, affiliated department, number of deliveries in the facility, and presence of midwifery outpatients and a maternity home in the hospital. In the second part of the questionnaire, as management skills that are required for middle managers in perinatal medicine, advanced midwives were asked to rate from 1 (exactly no) to 5 (exactly yes) regarding the necessity for each of 22 items at present and in the next generation (after 10-20 years) as shown in the appendix.
Statistical analyses
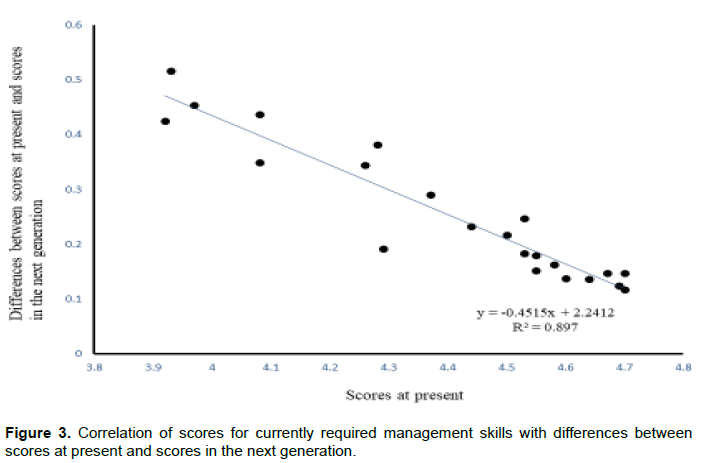
The differences and rates of changes between mean scores at present and those in the next generation were calculated. The differences between scores at present and those in the next generation were assessed by using the paired t-test. Correlations of scores for currently required management skills with the differences between scores at present and those in the next generation were analyzed by using Pearson’s coefficient correlation test. A two-sided value less than 0.05 was considered to be statistically significant. Multiple comparisons was applied by using Bonferroni’s correction, and the statistical threshold was adjusted to 0.0023 (0.05/22). All analyses were performed by using statistical package software (JMP® Pro ver.15.1.0).
Ethical consideration
This study was approved by the Ethics Committee of Tokushima University Hospital (Approval No. 3271). An anonymous questionnaire sheet was used in the survey. Each subject was provided with a research explanatory document setting out an explanation about the research and was informed that she would be deemed to consent to participation in the research by completing the questionnaire sheet and by checking in the check boxes. The consent of each subject was obtained on the basis of our explanation that participation in the survey was voluntary, that refusal to participate would cause no detrimental treatment, and that data obtained would not to be used for any purpose other than this research. With regard to the data, there were no statements or use of names by which personal information could be identified and all of the data were managed by numbers. Anonymity and privacy protection were ensured.
RESULTS
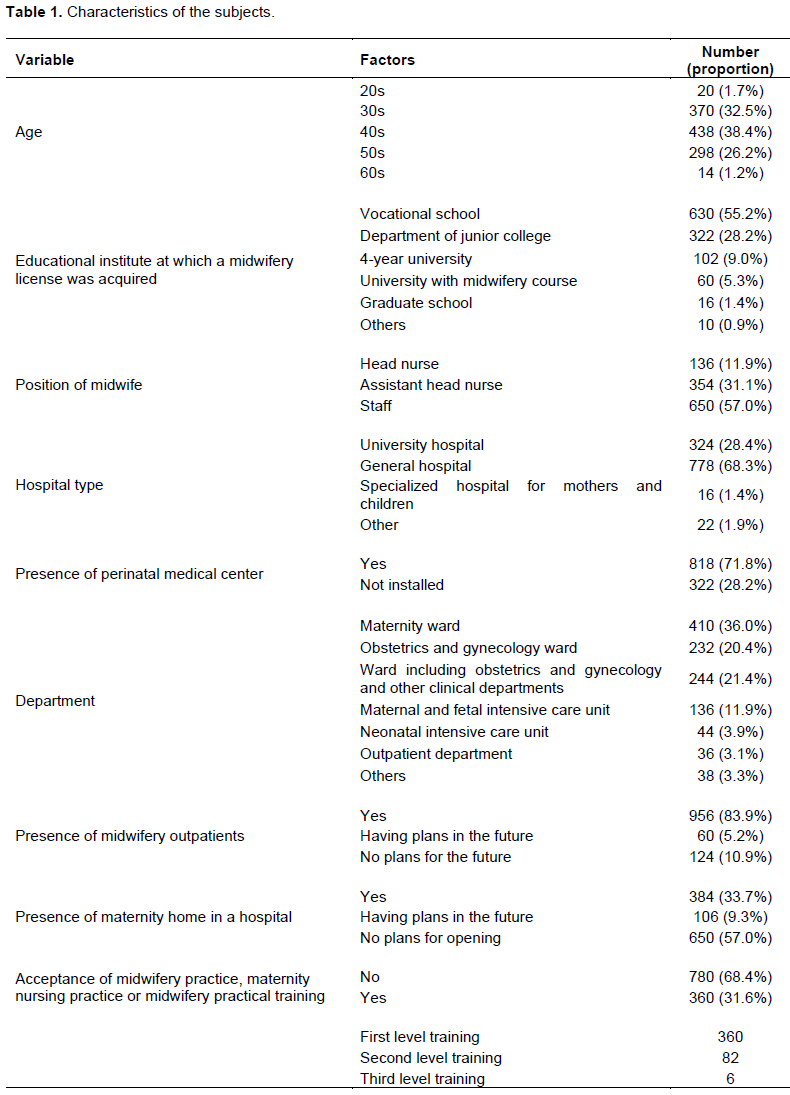
The demographics of the subjects are shown in Table 1. The mean period of midwifery experience was 19.1 years (ranging from 6 to 38 years), and the mean period in which midwives were head nurses was 5.3 years (ranging from 0.9 to 25 years). The mean number of labors between 2015 and 2017 was 638.1 (ranging from 10 to 1700). The proportion of subjects who responded that there had been an increase in the number of labors in the past 5 years was 20.3% (n=232) and the proportion of subjects who responded that there had been a decrease in the number of labors in the past 5 years was 43.0% (n=490).
Assessment of management skills currently required for middle managers
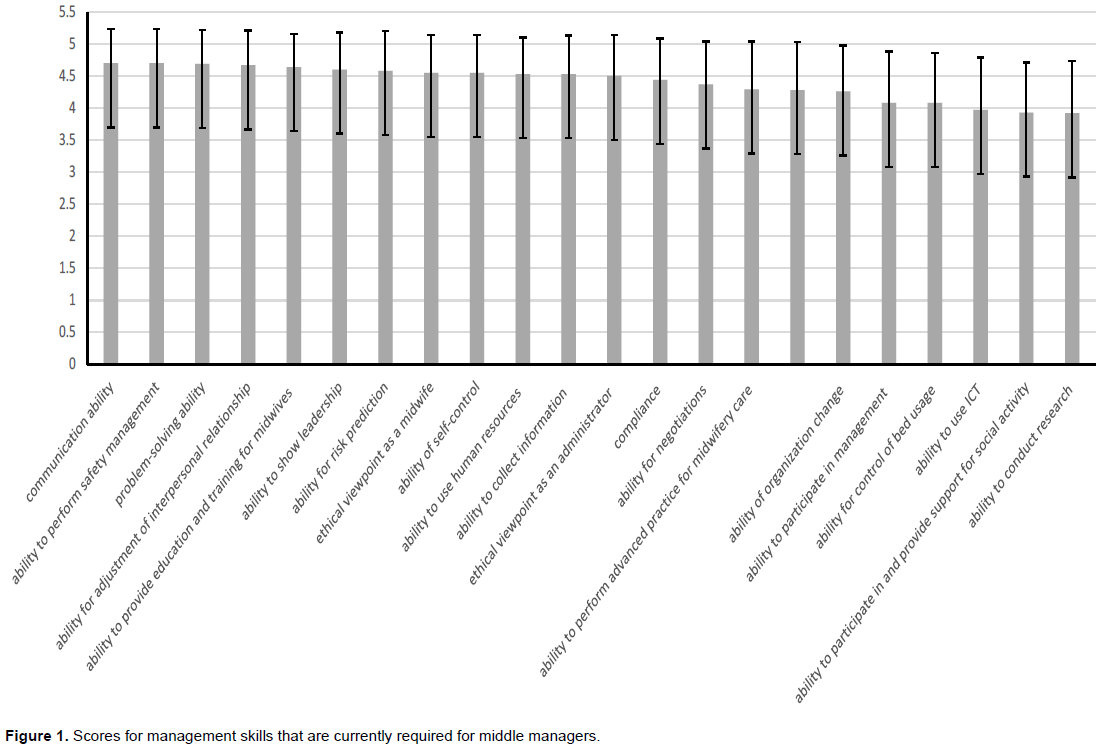
Management skills currently required for middle managers that were given high scores were communication ability, ability to perform safety management, problem-solving ability, ability for adjustment of interpersonal relationships, ability to provide education and training for midwives, ability to show leadership and ability for risk prediction (Figure 1).
Assessment of management skills required for middle managers in the next generation
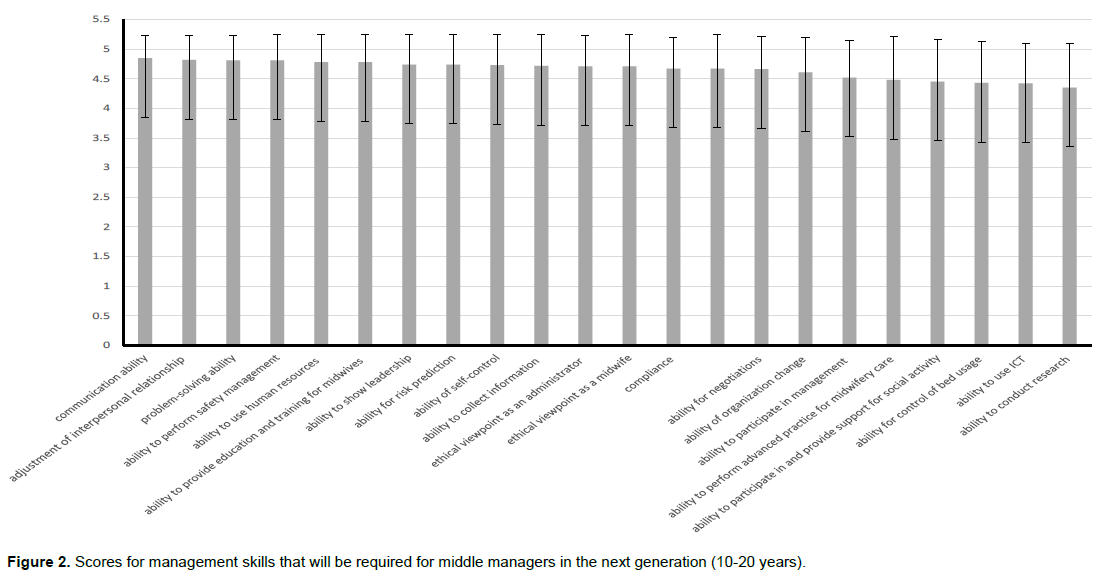
Management skills required for middle managers in the next generation that were given high scores were communication ability, ability for adjustment of interpersonal relationships, ability to perform safety management, problem-solving ability, ability to provide education and training for midwives, ability to use human resources, ability to show leadership, and ability for risk prediction (Figure 2). Of the top 7 items for management skills in the next generation, 6 items were the same as those with high scores for currently required management skills.
Differences between scores at present and scores in the next generation
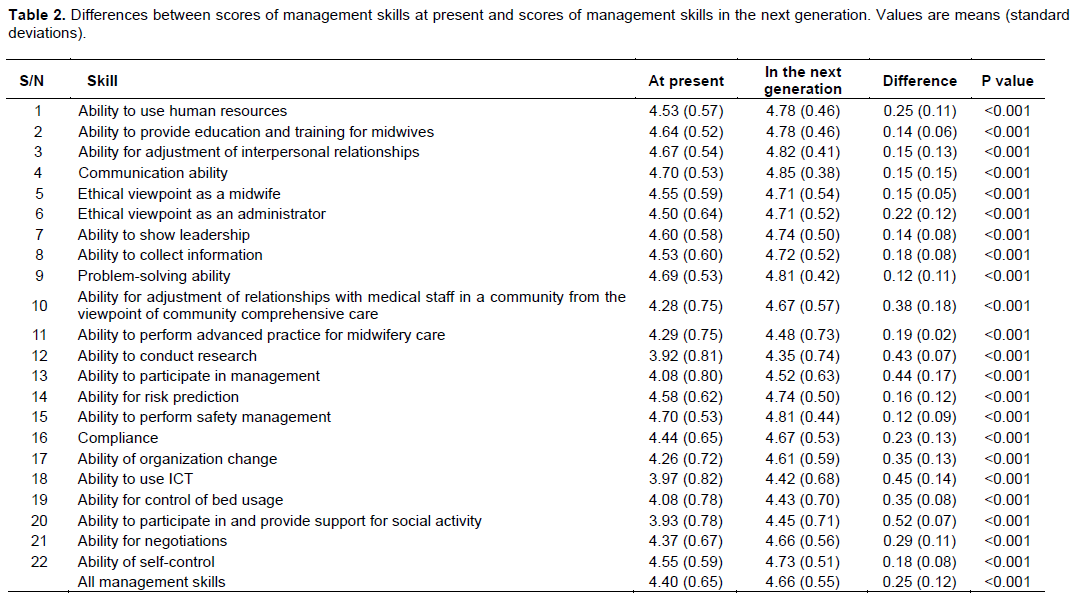
As can be seen in Table 2, the mean score (± standard deviation: SD) for all of the management skills currently required for middle managers was 4.40 (± 0.65) and the mean score (± SD) for all of the management skills required for middle managers in the next generation was 4.66 (± 0.55). Mean scores for management skills in the next generation were significantly higher than the mean scores for currently required management skills for all management skills (p<0.001). The items with high scores for currently required management skills and further increased scores for management skills in the next generation were communication ability, ability for adjustment of interpersonal relationships, ability to perform safety management, problem-solving ability, ability to provide education and training for midwives and ability to show leadership. The items with large differences between scores at present and scores in the next generation were ability to participate in social activity, ability to use ICT, ability to participate in management, ability to conduct research, ability for adjustments of relationships with medical staff in a community from the viewpoint of community comprehensive care, ability for organization change and ability for control of bed usage. Higher scores at present indicated smaller differences between scores at present and scores in the next generation. On the other hand, lower scores at present indicated larger differences between scores at present and scores in the next generation. Thus, as shown in Figure 3, there was a significant negative correlation of the scores for currently required management skills with differences between scores at present and scores in the next generation (r=-0.947, p<0.05).
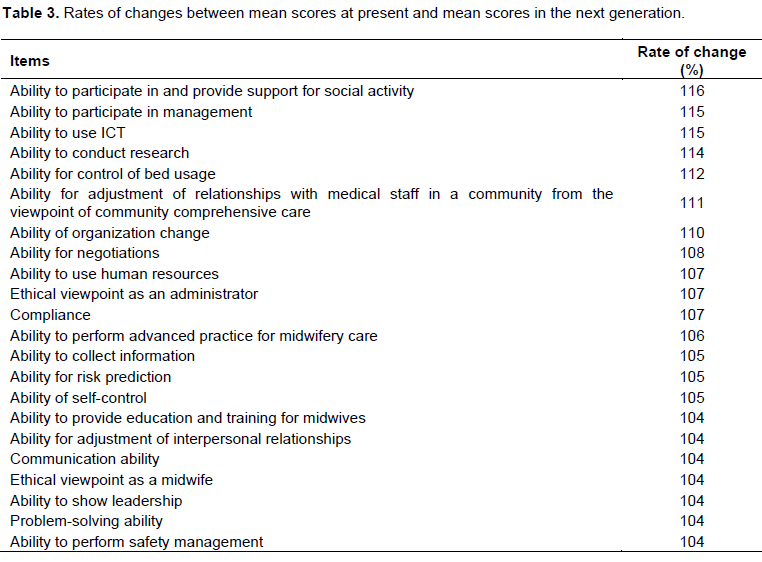
Rates of changes between mean scores at present and mean scores in the next generation
The rates of changes between mean scores at present and mean scores in the next generation are shown in Table 3. The rates of changes increased in all items. The items with large rates of change were ability to participate in social activity followed by ability to participate in management, ability to use ICT and ability to conduct research. The rates of changes in items that had high scores at present were small and, conversely, the rates of changes in items that had low scores at present were large.
DISCUSSION
In summary, all of the scores of items required in the next generation were significantly higher than those required at present. Items with high scores at present had high scores in the next generation and items with low scores at present showed remarkable increases in the next generation. It was shown that management skills for which high scores were given at present including communication ability, ability to perform safety management, problem-solving ability and ability for adjustment of interpersonal relationships were also important in the next generation. On the other hand, the scores given for ability for participation in social activity, ability to use ICT and ability to participate in management were low at present but high in the next generation.
These management skills showed very large differences and large rates of changes between scores at present and scores in the next generation. These findings have not been shown in previous studies. Given that perinatal care and nursing will change in the future, advanced midwives recognize that these skills are important.
A high level of communication ability is needed to establish good relationships with pregnant women and their families and for cooperation with medical staff. It is expected that the establishment of a working environment in which free communication is possible will lead to better cooperation among members of a medical team and will contribute to improvement in medical safety. It has been suggested that it is necessary for middle managers to provide a safe and secure medical environment by the establishment of good relationships with pregnant women and their family through a high level of communication ability (Nambu et al., 2006). Middle managers can cooperate with medical staff through their ability for adjustment of interpersonal relationships in a medical team as well as a high level of communication ability.
A middle manager must analyze causes of incidents that could have led to medical accidents, make an improvement plan for prevention of recurrence and assess the plan as a risk manager. Since education for risk management has not been sufficient for fundamental nursing education in a university, midwives have learned risk management through their clinical experiences. It was suggested that risk management is important for ensuring the safety of pregnant women and postpartum women and that the introduction of an educational program for risk management is necessary in nursing education in Australia (Johnstone and Kanitsaki, 2007). It was proposed by the International Confederation of Midwives that physical and mental health problems are background factors of child maltreatment and that physical violence and sexual violence are linked to low-birth-weight babies, miscarriage, stillbirth and maternal death. It has been suggested that midwives all over the world should encourage women and children to participate in available follow-up programs (International Confederation of Midwives, 2020). Hattori (2019) suggested that midwives with a high level of ability for performing safety management would be able to detect risks such as risks of abuse and neglect when they feel that something is wrong based on their experiences in the process of providing midwifery care for women before and after delivery. As a problem-solving ability, middle managers need to obtain medical and social information for postpartum women with those risks and assess their risks until they leave the hospital after delivery. Since cases of abuse, neglect and sudden delivery and the number of pregnant women with psychological diseases are increasing (Franziska and Fanny, 2016), advanced midwives may consider that management skills for these cases are important in the future.
The scores given for the ability for participation in social activity, ability to use ICT and ability to participate in management were low at present but high in the next generation. These management skills showed very large differences and large rates of changes between scores at present and scores in the next generation. The places where medical care are provided will shift from hospitals to communities or home healthcare, and the establishment of community-based integrated care systems has been promoted in Japan (Umino, 2020). In the United Kingdom, postpartum women can raise their child with confidence since they receive midwifery care by the same midwife from delivery until the postpartum period (Kirkham?2003). However, in Japan, midwives in a hospital cannot continue to provide midwifery care after delivery. It has been reported that midwives in a hospital provide information to midwives in a community when postpartum women return home from the hospital, but cooperation between midwives in a hospital and midwives in a community is insufficient (Maeda, 2007). Kasai et al. (2018) suggested that continuous midwifery care for postpartum women was effective for prevention of depression, suicide and abuse in postpartum women.
Middle managers in the next generation will need to establish a system in which advanced midwives in a hospital can act outside the hospital.
Recently, the use of ICT in medical care has been increasing in Japan (Yoshimura, 2018). Early detection of an abnormality in pregnant women by using ICT is important for preventing risks of death in pregnant women and fetuses and for improving fetal life prognosis. By the use of a mobile fetal heart rate monitoring device, a system in which an obstetrician in a hospital can assess the status of well-being in fetuses of pregnant women in remote areas has recently been established (Ogasawara et al., 2015). A support system for pregnant women in which medical staff can cooperate with each other through data in electronic medical records in a perinatal medical information network has also recently been established (Ministry of Health, Labour and Welfare, 2018). Since utilization of ICT will progress, basic knowledge about ICT and practice of ICT utilization are needed for midwives. In New Zealand, midwives use ICT for various purposes including clinical practice, dissemination of evidence-based information, communication with pregnant women and their families, education and professional development (Knight and Stewart, 2010). Middle managers in the next generation may need to utilize ICT from the viewpoint of midwifery care and may need to strengthen cooperation with obstetricians and medical staff.
Advanced midwives required the ability to participate in management as middle managers in the next generation. It has been reported that a decrease in overtime work resulted in maintenance of the work-life balance and that its effect was related to the prevention of turnover of midwives (Endo and Yamada, 2019). Maintenance of the number of advanced midwives may contribute to hospital management through high levels of satisfaction of pregnant women and postpartum women due to enrichment of midwifery care.
This study had a large sample size. The subjects consisted of advanced midwives with various background characteristics. However, the subjects in the present study were advanced midwives working in hospitals that have more than 300 beds and the study did not include advanced midwives working in hospitals that have less than 300 beds. Management skills may be different depending on the scale and function of hospitals in which midwives are working. Further study on advanced midwives who work in moderate-scaled hospitals and in maternity homes is needed.
CONCLUSION
Advanced midwives consider that management skills required for middle managers will change in the future. Middle managers will need to ensure that midwifery care can be provided not only in a hospital but also in a community and strengthen cooperation between midwives in a community and public health nurses. Middle managers will also need to consider perinatal medicine and nursing from various points of view such as utilization of ICT and participation in management.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors express deep gratitude to the advanced midwives who participated in this study and there was no funding for the study.
REFERENCES
|
Abe M, Yasui T, Matsuura Y, Hake M (2020). Management skills required for nursing middle managers in the next generation in perinatal medical care. International Journal of Nursing and Midwifery 12(4):151-157. |
|
|
Asano Y, Hirai H, Nakayama K (2018). Literature review on support using the Edinburgh Postnatal Depression Scale (EPDS). Niigata Journal of Health and Welfare 18(2):6-12. |
|
|
Endo C, Yamada S (2019). Relationship between burnout and burden of responsibility of midwives in maternity wards. Journal of the Japan Academy of Nursing Administration and Policies 23(1):92-102. |
|
|
Franziska U, Fanny P (2016). Consequences and Possible Predictors of Health-damaging Behaviors and Mental Health Problems in Pregnancy - A Review 76(11):1136-1156. |
|
|
Goemaes R, Beeckman D, Goossens J, Shawe J, Verhaeghe S, Hecke AV (2016). Advanced midwifery practive: An evolutionary concept analysis. Midwifery 42:29-37. |
|
|
Guille C, Newman R, Fryml LD, Lifton CK, Epperson CN (2013). Management of postpartum depression. Journal of Midwifery and Women's Health 58:643-653. |
|
|
Harada H, Yamashita T, Susaki S, Nakashima E, Tukahara H (2014). Survey of the early select education to next-generation leaders. The Japanese Association of Medical and Nursing Education 23(1):33-37. |
|
|
Hattori R (2019). Research on Midwives Recognized "Mothers and their children in need of concern" and collaboration with other agencies. Journal of Gifu College of Nursing 19(1):63-73. |
|
|
Hutchens BE, Learney J (2020). Risk factors for postpartum depression: an umbrella review. Journal of Midwifery and Women's Health 65(1):96-108. |
|
|
Ibe T, Yamada M, Matsumoto N, Oku H, Nakamura A, Fukuda M, Yoshida C (2012). How should we develop competent nurse administrators? Proposal to revise Japanese Nursing Association's certified nurse administrator education protocols. Bulletin of St. Luke's College of Nursing 38:63-70. |
|
|
Inoue H (2014). Management competency of nurse manager. Kochi Women's University Academy of Nursing 40(1):109-116. |
|
|
International Confederation of Midwives (2020). |
|
|
Japan Nursing Association (2013). Guidelines for applying clinical ladder of competencies for midwifery practice (CLoCMip?). Excerpted version (English Translation) pp. 1-38. |
|
|
Japan Nursing Association (2016). |
|
|
Johnstone MJ, Kanitsaki O (2007). Clinical risk management and patient safety education for nurses: a critique. Nurse Education Today 27(3):185-191. |
|
|
Kasai K, Yamashiro S, Tamura C, Kitame T, Watanabe K, Takehara K (2018). Mental health of primipara mothers within one month of childbirth observed by midwives through newborn visits. Journal of Japan Academy of Midwifery 32(1):27-36. |
|
|
Katz RL (1974). Skills of an effective administrator. Harvard Business Review 52:90-102. |
|
|
Kirkham M (2003). Birth Centers: A Social Model for Maternity Care. Books for Midwives Elsevier Science Limited. |
|
|
Kitajima H (2008). Relationship between nursing care in mixed obstetrics-only wards at large hospitals in Japan and the frequency of MRSA infection in neonates. Japanese Journal of Environmental Infections 23(2):129-134. |
|
|
Knight D, Stewart S (2010). Midwives and technology: The Case from New Zealand. Health Management 5:1-7. |
|
|
Maeda K (2007). The clinical competency required by the nurse and the midwife working with child abuse cases in the maternity unit and the NICU: nurses' and midwive's experiences and perceptions in Okinawa. Journal of Okinawa Prefectural College of Nursing 8:39-47. |
|
|
Ministry of Health, Labour and Welfare (2019). |
|
|
Moriyama M, Hunashima N (2015). Desirable behavior of head nurses through their perception. Japan Academic Society of Nursing Education 24(1):57-68. |
|
|
Motomura M, Kawaguchi T (2013). Development of a nursing administrator's competency assessment scale (NACAS) for nursing administrator in mid-size hospitals. Japanese Journal of Nursing Research 36(1):61-70. |
|
|
Nambu M, Harada E, Suto S (2006). Risk sharing communication in medical setting: An analyses of nurses' conversation: Cognitive Studies. Bulletin of the Japanese Cognitive Science Society 13(1):62-79. |
|
|
Ogasawara T, Yamada T, Kawataki M, Hiromatsu H, Takeuti Y, Hara H (2015). Dissemination and prospects of new perinatal telemedicine and perinatal ICT. Japanese Journal of Telemedicine and Telecare 11(2):160-163? |
|
|
Ohira M, Imada Y, Nagami K (2007). Public-nurses' perspective on the relationship between public health-nurses and midwifes for maternal care. Journal of Mie Prefectural College of Nursing 11:9-19. |
|
|
Suzuki S, Muranaka Y (2018). Development of a competency rating scale for head nurses in realization of work-life balance among nurses. Juntendo University Journal of Health Care and Nursing 14(2):30-41. |
|
|
Teraoka A, Saito I, Saaya T, Sato S (2019). Nursing time and activities during delivery period in cooperation with midwives and nurses in mixed wards. Journal of Japan Academy of Midwifery 33(1):82-91. |
|
|
Umino K (2020). A review of nurse competency required by the community-based integrated care system. Tokiwa Journal of Nursing Research 2:63-73. |
|
|
Yoshimura K (2018). Current status of ICT policy at the ministry of health, labor and welfare. Journal of National Institute of Public Health 67(2):158-165. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


